
Page 5 - UHL Term 2017
P. 5
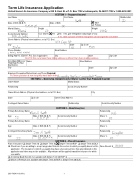
Term Life Insurance Application
United Home Life Insurance Company 225 S. East St. P.O. Box 7192 Indianapolis, IN 46207-7192 1-800-428-3001
SECTION 1 – Proposed Insured
FirstName Smith StateofBirth TX
Height 6'0
Last Name
John Married
Middle Initial
D
Date of Birth (M-D-Y)5/5/1965
Male Female
Marital Status
Weight 200lbs U.S.Citizen: Yes No Ifno,giveimmigrationstatus/typeofvisa:
SocialSecurityNumber
555-21-3456
Street Address (Physical street address, not a P.O. Box) 123 Easy St.
If no, take a picture of there visa/green card and get the id number
ZipCode75001 State
Don't fill this out unless there billing address is differnt then there mailing address
Secondary Addressee/ Street Address Third Party (For Past
Due Notices)
City
Employer/Occupation/Duties/How Long There (Required) Accounting Firm Inc./ accountant/ 5years Put there posistion & how long they have been there
City Dallas
Phone Number Email Address
State
( 555) 555-5555
Billing Address (Owner’s P.O. Box if applicable) City
TX
Zip Code
Zip Code
Name
SECTION 2 – Ownership (Complete only if Owner is other than Proposed Insured)
Owner Name
Relationship
Owner Street Address (Physical street address, not a P.O. Box)
Marital Status
Social Security Number
State
City
State
Contingent Owner Name
Primary Beneficiary NameMary A. Smith
Age 52
Primary Beneficiary Name Age
Contingent Beneficiary Name Age
Owner Email Address
Social Security Number Relationship Wife
Zip Code
Relationship
SECTION 3 – Beneficiary(ies)
Social Security Number
Date of Birth (M-D-Y)
Social Security Number
Social Security Number
Date of Birth (M-D-Y)
Share %
Relationship
Share %
Relationship Daughter Share %
01-01-1965
100 100
Jane A. Smith
Date of Birth (M-D-Y)
22 02-01-1995 SECTION4–PlanofInsurance
Plan of Insurance Simple Term 20 Simple Term 30 Simple Term 20 ROP Simple Term 20 DLX Check here if you are willing to accept any product listed in this section for which you qualify based on this
100,000
application. The insurance for which you qualify may have a face amount less than any indicated on this application and riders may not be available. All premiums will be applied toward the insurance for which you qualify.
Accidental Death Benefit (not available with Simple Term 20 ROP) $ ____________________ Waiver of Premium (not available with Simple Term 20 ROP or Simple Term 20 DLX)
Face Amount: $__________________
200-783A 9-16 (NV) 1
