
Page 15 - ABC Company 2018 Open Enrollment Guide
P. 15
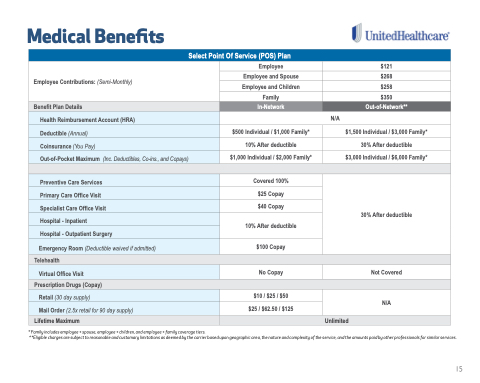
Medical Benefits
Select Point Of Service (POS) Plan
Employee Contributions: (Semi-Monthly)
Employee
$121
Employee and Spouse
$268
Employee and Children
$258
Family
$350
Benefit Plan Details
In-Network
Out-of-Network**
Health Reimbursement Account (HRA)
N/A
Deductible (Annual)
$500 Individual / $1,000 Family*
$1,500 Individual / $3,000 Family*
Coinsurance (You Pay)
10% After deductible
30% After deductible
Out-of-Pocket Maximum (Inc. Deductibles, Co-ins., and Copays)
$1,000 Individual / $2,000 Family*
$3,000 Individual / $6,000 Family*
Preventive Care Services
Covered 100%
30% After deductible
Primary Care Office Visit
$25 Copay
Specialist Care Office Visit
$40 Copay
Hospital - Inpatient
10% After deductible
Hospital - Outpatient Surgery
Emergency Room (Deductible waived if admitted)
$100 Copay
Telehealth
Virtual Office Visit
No Copay
Not Covered
Prescription Drugs (Copay)
Retail (30 day supply)
$10 / $25 / $50
N/A
Mail Order (2.5x retail for 90 day supply)
$25 / $62.50 / $125
Lifetime Maximum
Unlimited
* Family includes employee + spouse, employee + children, and employee + family coverage tiers.
* *Eligible charges are subject to reasonable and customary limitations as deemed by the carrier based upon geographic area, the nature and complexity of the service, and the amounts paid by other professionals for similar services.
15
