
Page 12 - IPsoft 2018 Benefits Guide
P. 12
12
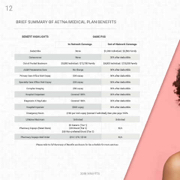
BRIEF SUMMARY OF AETNA MEDICAL PLAN BENEFITS
BENEFIT HIGHLIGHTS
Deductible
Out-of-Pocket Maximum
OAMC POS
Specialty Care Of ce Visit Copay
In-Network Coverage
Primary Care Of ce Visit Copay $20 copay deductible
Complex Imaging $50 copay deductible
Diagnostic X-Ray/Labs Covered 100% deductible
Emergency Room $100 per visit copay (waived if admitted), then plan pays 100%
$5 Generic (Tier 1)
Pharmacy Copays (Retail Store) $35 Brand (Tier 2) N/A
$60 Non-preferred Brand (Tier 3)
Please refer to full Summary of Bene ts enclosure for fee schedule for more services.
None
$20 copay
Out-of-Network Coverage
$1,000 Individual / $2,500 Family
Coinsurance
None
Adult Preventative Care
$5,080 Individual / $12,700 Family $4,000 Individual / $10,000 Family
No Charge
30% after
30% after
deductible
30% after
deductible
30% after
deductible
Covered 100%
30% after
Hospital Outpatient
30% after
deductible
30% after
Hospital Inpatient
$500 copay
2018 Benefits
30% after deductible
Lifetime Maximum
Unlimited
Unli
mited
Pharmacy Copays Mail Order
$10 / $70 / $120
N/A
