
Page 18 - Demo
P. 18
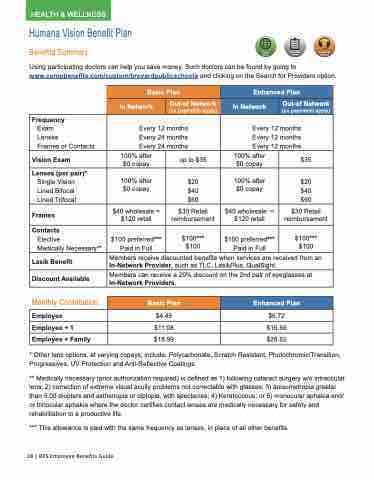
Humana Vision Benefit Plan
Benefits Summary
Online Important Tools Forms
Using participating doctors can help you save money. Such doctors can be found by going to www.compbenefits.com/custom/brevardpublicschools and clicking on the Search for Providers option.
Customer Service
Basic Plan
Enhanced Plan
In Network
Out-of Network
(co payments apply)
In Network
Out-of Network
(co payments apply)
Frequency
Exam
Lenses
Frames or Contacts
Every 12 months Every 24 months Every 24 months
Every 12 months Every 12 months Every 12 months
Vision Exam
100% after $0 copay
up to $35
100% after $0 copay
$35
Lenses (per pair)*
Single Vision Lined Bifocal Lined Trifocal
100% after $0 copay
$20 $40 $60
100% after $0 copay
$20 $40 $60
Frames
$40 wholesale = $120 retail
$30 Retail reimbursement
$40 wholesale = $120 retail
$30 Retail reimbursement
Contacts
Elective
Medically Necessary**
$100 preferred*** Paid in Full
$100*** $100
$100 preferred*** Paid in Full
$100*** $100
Lasik Benefit
Members receive discounted benefits when services are received from an In-Network Provider, such as TLC, LasikPlus, QualSight.
Discount Available
Members can receive a 20% discount on the 2nd pair of eyeglasses at In-Network Providers.
Monthly Contribution
* Other lens options, at varying copays, include: Polycarbonate, Scratch Resistant, Photochromic/Transition, Progressives, UV Protection and Anti-Reflective Coatings.
** Medically necessary (prior authorization required) is defined as 1) following cataract surgery w/o intraocular lens; 2) correction of extreme visual acuity problems not correctable with glasses; 3) anisometropia greater than 5.00 diopters and asthenopia or diplopia, with spectacles; 4) Keratoconus; or 5) monocular aphakia and/ or binocular aphakia where the doctor certifies contact lenses are medically necessary for safety and rehabilitation to a productive life.
*** This allowance is paid with the same frequency as lenses, in place of all other benefits.
Basic Plan
Enhanced Plan
Employee
$4.45
$6.72
Employee + 1
$11.08
$16.69
Employee + Family
$18.99
$28.62
18 | BPS Employee Benefits Guide
HEALTH & WELLNESS
