
Page 3 - Golden Dental Plans – HealthChoice Small Business Dental Program
P. 3
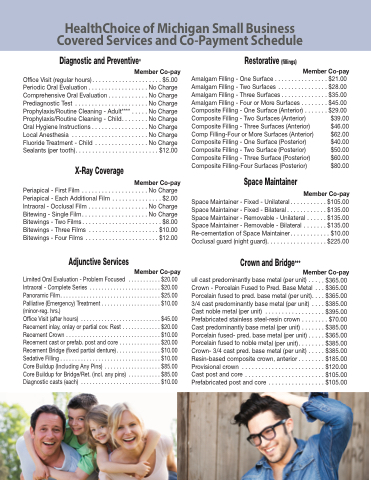
HealthChoice of Michigan Small Business Covered Services and Co-Payment Schedule
Diagnostic and Preventive*
Member Co-pay
Office Visit (regular hours) . . . . . . . . . . . . . . . . . . . . . $5.00 Periodic Oral Evaluation . . . . . . . . . . . . . . . . . . No Charge Comprehensive Oral Evaluation . . . . . . . . . . . . No Charge Prediagnostic Test . . . . . . . . . . . . . . . . . . . . . . No Charge Prophylaxis/Routine Cleaning - Adult**** . . . . . No Charge Prophylaxis/Routine Cleaning - Child. . . . . . . . No Charge Oral Hygiene Instructions . . . . . . . . . . . . . . . . . No Charge Local Anesthesia . . . . . . . . . . . . . . . . . . . . . . . No Charge Fluoride Treatment - Child . . . . . . . . . . . . . . . . No Charge Sealants (per tooth). . . . . . . . . . . . . . . . . . . . . . . . . $12.00
Restorative (fillings)
Periapical - First Film . . . . . . . . . Periapical - Each Additional Film Intraoral - Occlusal Film . . . . . . . Bitewing - Single Film. . . . . . . . . Bitewings - Two Films . . . . . . . . . Bitewings - Three Films . . . . . . . Bitewings - Four Films . . . . . . . .
Member Co-pay
. . . . . . . . . . . No Charge . . . . . . . . . . . . . . . $2.00 . . . . . . . . . . . No Charge . . . . . . . . . . . No Charge . . . . . . . . . . . . . . . $8.00 . . . . . . . . . . . . . . $10.00 . . . . . . . . . . . . . . $12.00
Member Co-pay
X-Ray Coverage
Adjunctive Services
Space Maintainer - Fixed - Unilateral. . . . . . . . . . . $105.00 Space Maintainer - Fixed - Bilateral . . . . . . . . . . . . $135.00 Space Maintainer - Removable - Unilateral . . . . . . $135.00 Space Maintainer - Removable - Bilateral . . . . . . . $135.00 Re-cementation of Space Maintainer . . . . . . . . . . . . $10.00 Occlusal guard (night guard). . . . . . . . . . . . . . . . . . $225.00
Crown and Bridge***
Member Co-pay
ull cast predominantly base metal (per unit) . . . . . $365.00 Crown - Porcelain Fused to Pred. Base Metal . . . $365.00 Porcelain fused to pred. base metal (per unit). . . . $365.00 3/4 cast predominantly base metal (per unit) . . . . $385.00 Castnoblemetal(perunit) ..................$395.00 Prefabricated stainless steel-resin crown . . . . . . . . $70.00 Cast predominantly base metal (per unit) . . . . . . . $385.00 Porcelain fused- pred. base metal (per unit) . . . . . $365.00 Porcelain fused to noble metal (per unit) . . . . . . . . $385.00 Crown- 3/4 cast pred. base metal (per unit) . . . . . $385.00 Resin-based composite crown, anterior . . . . . . . . $185.00 Provisionalcrown .........................$120.00 Castpostandcore ........................$105.00 Prefabricatedpostandcore .................$105.00
Limited Oral Evaluation - Problem Focused Intraoral - Complete Series . . . . . . . . . . . . . Panoramic Film. . . . . . . . . . . . . . . . . . . . . . . Palliative (Emergency) Treatment . . . . . . . . . (minor-reg. hrs.)
Office Visit (after hours) . . . . . . . . . . . . . . . . Recement inlay, onlay or partial cov. Rest . . Recement Crown . . . . . . . . . . . . . . . . . . . . . Recement cast or prefab. post and core . . . Recement Bridge (fixed partial denture) . . . . Sedative Filling . . . . . . . . . . . . . . . . . . . . . . . Core Buildup (Including Any Pins) . . . . . . . . Core Buildup for Bridge/Ret. (incl. any pins) Diagnostic casts (each) . . . . . . . . . . . . . . . .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
Member Co-pay
. . . . . . . . . $20.00 . . . . . . . . . $20.00 . . . . . . . . . $25.00 . . . . . . . . . $10.00
. . . . . . . . . $45.00 . . . . . . . . . $20.00 . . . . . . . . . $10.00 . . . . . . . . . $20.00 . . . . . . . . . $10.00 . . . . . . . . . $10.00 . . . . . . . . . $85.00 . . . . . . . . . $85.00 . . . . . . . . . $10.00
Amalgam Filling - One Surface . . . . . . . . . . . Amalgam Filling - Two Surfaces . . . . . . . . . . Amalgam Filling - Three Surfaces . . . . . . . . . Amalgam Filling - Four or More Surfaces . . . Composite Filling - One Surface (Anterior) . . Composite Filling - Two Surfaces (Anterior) Composite Filling - Three Surfaces (Anterior) Comp Filling-Four or More Surfaces (Anterior) Composite Filling - One Surface (Posterior) Composite Filling - Two Surface (Posterior) Composite Filling - Three Surface (Posterior) Composite Filling-Four Surfaces (Posterior)
Space Maintainer
Member Co-pay
. . . . .
. . . . $21.00 . . . . $28.00 . . . . $35.00 . . . . $45.00 . . . . $29.00
$39.00 $46.00 $62.00 $40.00 $50.00 $60.00 $80.00
