
Page 12 - HCSC2019EG
P. 12
10
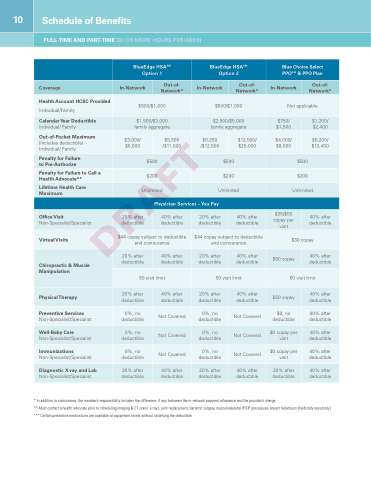
Schedule of Benefits
FULL-TIME AND PART-TIME (30 OR MORE HOURS PER WEEK)
BlueEdge HSASM Option 1
BlueEdge HSASM Option 2
Blue Choice Select PPOSM & PPO Plan
Coverage
In-Network
Out-of- Network*
In-Network
Out-of- Network*
In-Network
Out-of- Network*
Health Account HCSC Provided
Individual/Family
$500/$1,000
$500/$1,000
Not applicable
Calendar Year Deductible
Individual/ Family
$1,500/$3,000 family aggregate
$2,500/$5,000 family aggregate
$750/ $1,500
$1,200/ $2,400
Out-of-Pocket Maximum
(includes deductible) Individual/ Family
$3,000/ $6,000
$5,500 /$11,000
$6,250 /$12,500
$12,500/ $25,000
$4,000/ $8,000
$5,200/ $10,400
Penalty for Failure to Pre-Authorize
$500
$500
$500
Penalty for Failure to Call a Health Advocate**
$200
$200
$200
Lifetime Health Care Maximum
Unlimited
Unlimited
Unlimited
Physician Services –You Pay
Office Visit
Non-Specialist/Specialist
20% after deductible
40% after deductible
20% after deductible
40% after deductible
$35/$50 copay per visit
40% after deductible
Virtual Visits
$44 copay subject to deductible and coinsurance
$44 copay subject to deductible and coinsurance
$30 copay
Chiropractic & Muscle Manipulation
20% after deductible
40% after deductible
20% after deductible
40% after deductible
$50 copay
40% after deductible
50 visit limit
50 visit limit
50 visit limit
Physical Therapy
20% after deductible
40% after deductible
20% after deductible
40% after deductible
$50 copay
40% after deductible
Preventive Services
Non-Specialist/Specialist
0%, no deductible
Not Covered
0%, no deductible
Not Covered
$0, no deductible
40% after deductible
Well-Baby Care
Non-Specialist/Specialist
0%, no deductible
Not Covered
0%, no deductible
Not Covered
$0 copay per visit
40% after deductible
Immunizations
Non-Specialist/Specialist
0%, no deductible
Not Covered
0%, no deductible
Not Covered
$0 copay per visit
40% after deductible
Diagnostic X-ray and Lab
Non-Specialist/Specialist
20% after deductible
40% after deductible
20% after deductible
40% after deductible
20% after deductible
40% after deductible
* In addition to coinsurance, the member’s responsibility includes the difference, if any, between the in-network payment allowance and the provider’s charge.
** Must contact a health advocate prior to scheduling imaging & CT scans, x-rays, joint replacement, bariatric surgery, musculoskeletal IP/OP procedures, breast reductions (medically necessary). *** Certain preventive medications are available at copayment levels without satisfying the deductible.
