
Page 15 - HCSC2019EG
P. 15
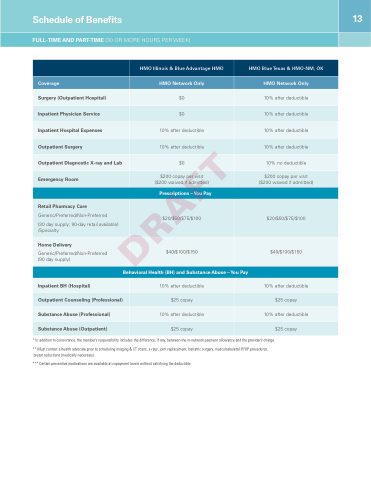
Schedule of Benefits
13
FULL-TIME AND PART-TIME (30 OR MORE HOURS PER WEEK)
HMO Illinois & Blue Advantage HMO
HMO Blue Texas & HMO-NM, OK
Coverage
HMO Network Only
HMO Network Only
Surgery (Outpatient Hospital)
$0
10% after deductible
Inpatient Physician Service
$0
10% after deductible
Inpatient Hospital Expenses
10% after deductible
10% after deductible
Outpatient Surgery
10% after deductible
10% after deductible
Outpatient Diagnostic X-ray and Lab
$0
10% no deductible
Emergency Room
$200 copay per visit ($200 waived if admitted)
$200 copay per visit ($200 waived if admitted)
Prescriptions –You Pay
Retail Pharmacy Care
Generic/Preferred/Non-Preferred
(30 day supply; 90-day retail available) /Specialty
$20/$50/$75/$100
$20/$50/$75/$100
Home Delivery
Generic/Preferred/Non-Preferred (90 day supply)
$40/$100/$150
$40/$100/$150
Behavioral Health (BH) and Substance Abuse – You Pay
Inpatient BH (Hospital)
10% after deductible
10% after deductible
Outpatient Counseling (Professional)
$25 copay
$25 copay
Substance Abuse (Professional)
10% after deductible
10% after deductible
Substance Abuse (Outpatient)
$25 copay
$25 copay
* In addition to coinsurance, the member’s responsibility includes the difference, if any, between the in-network payment allowance and the provider’s charge.
** Must contact a health advocate prior to scheduling imaging & CT scans, x-rays, joint replacement, bariatric surgery, musculoskeletal IP/OP procedures, breast reductions (medically necessary).
*** Certain preventive medications are available at copayment levels without satisfying the deductible.
