
Page 9 - QARANC Vol 16 No 1 2018
P. 9
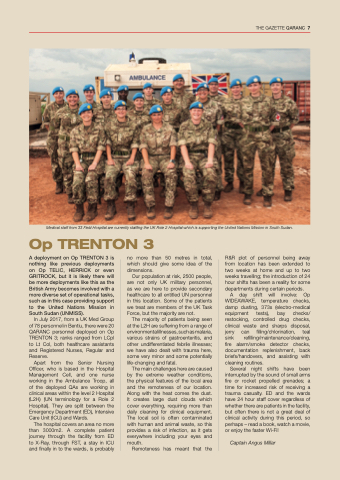
Medical staff from 33 Field Hospital are currently staffing the UK Role 2 Hospital which is supporting the United Nations Mission in South Sudan.
Op TRENTON 3
A deployment on Op TRENTON 3 is nothing like previous deployments on Op TELIC, HERRICK or even GRITROCK, but it is likely there will be more deployments like this as the British Army becomes involved with a more diverse set of operational tasks, such as in this case providing support to the United Nations Mission in South Sudan (UNMISS).
In July 2017, from a UK Med Group of 78 personnel in Bentiu, there were 20 QARANC personnel deployed on Op TRENTON 3; ranks ranged from LCpl to Lt Col, both healthcare assistants and Registered Nurses, Regular and Reserve.
Apart from the Senior Nursing Officer, who is based in the Hospital Management Cell, and one nurse working in the Ambulance Troop, all of the deployed QAs are working in clinical areas within the level 2 Hospital (L2H) (UN terminology for a Role 2 Hospital). They are split between the Emergency Department (ED), Intensive Care Unit (ICU) and Wards.
The hospital covers an area no more than 3000m2. A complete patient journey through the facility from ED to X-Ray, through FST, a stay in ICU and finally in to the wards, is probably
no more than 50 metres in total, which should give some idea of the dimensions.
Our population at risk, 2500 people, are not only UK military personnel, as we are here to provide secondary healthcare to all entitled UN personnel in this location. Some of the patients we treat are members of the UK Task Force, but the majority are not.
The majority of patients being seen at the L2H are suffering from a range of environmental illnesses, such as malaria, various strains of gastroenteritis, and other undifferentiated febrile illnesses; we have also dealt with trauma here, some very minor and some potentially life-changing and fatal.
The main challenges here are caused by the extreme weather conditions, the physical features of the local area and the remoteness of our location. Along with the heat comes the dust. It creates large dust clouds which cover everything, requiring more than daily cleaning for clinical equipment. The local soil is often contaminated with human and animal waste, so this provides a risk of infection, as it gets everywhere including your eyes and mouth.
Remoteness has meant that the
R&R plot of personnel being away from location has been extended to two weeks at home and up to two weeks travelling; the introduction of 24 hour shifts has been a reality for some departments during certain periods.
A day shift will involve: Op WIDEAWAKE, temperature checks, damp dusting, 373s (electro-medical equipment tests), bay checks/ restocking, controlled drug checks, clinical waste and sharps disposal, jerry can filling/chlorination, teal sink refilling/maintenance/cleaning, fire alarm/smoke detector checks, documentation replenishment, back briefs/handovers, and assisting with cleaning routines.
Several night shifts have been interrupted by the sound of small arms fire or rocket propelled grenades; a time for increased risk of receiving a trauma casualty. ED and the wards have 24 hour staff cover regardless of whether there are patients in the facility, but often there is not a great deal of clinical activity during this period, so perhaps – read a book, watch a movie, or enjoy the faster Wi-Fi!
Captain Angus Millar
THE GAZETTE QARANC 7
