
Page 20 - SAPOA COVID19 Restaurant Guidelines
P. 20
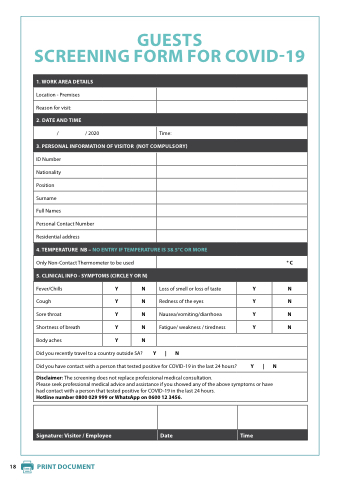
GUESTS
SCREENING FORM FOR FOR COVID-19
1 WORK AREA DETAILS
Location - Premises
Reason for visit:
2 DATE AND TIME
/ / / / 2020
Time:
3 PERSONAL INFORMATION OF VISITOR (NOT COMPULSORY)
ID Number
Nationality
Position
Surname
Full Names
Personal Contact Number
Residential address
4 TEMPERATURE TEMPERATURE NB – NO ENTRY IF TEMPERATURE TEMPERATURE IS 38 5°C OR OR MORE
Only Non-Contact Thermometer to be used
°C 5 CLINICAL INFO - SYMPTOMS (CIRCLE Y Y OR N)
Fever/Chills
Y N Loss of of smell or loss of of taste
Y N Cough
Y N Redness of the eyes
Y N Sore throat
Y N Nausea/vomiting/diarrhoea
Y N Shortness of breath
Y N Fatigue/ weakness / / tiredness
Y N Body aches
Y N Did you recently travel to a a country outside SA? Y | N Did you have contact with a a a a a person that tested positive for COVID-19
in the last 24 hours? Y | N Disclaimer: The screening does not replace professional professional medical medical consultation Please seek professional professional medical medical advice and assistance if you showed any of of of the the above symptoms or or have had contact with a a a a a a a a a a a a a a person that tested positive for COVID-19
in in the the last 24 hours Hotline number 0800 029 999 or or WhatsApp on on on 0600 12 3456 Signature: Visitor / Employee
Date
Time 18 PRINT DOCUMENT PRINT DOCUMENT
