
Page 19 - Horizons Manual
P. 19
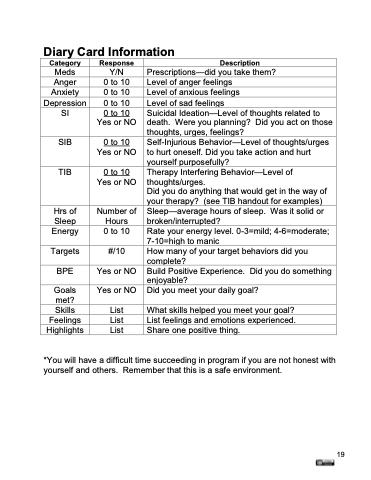
Diary Card Information
Category
Meds Anger Anxiety Depression
Response
Y/N 0 to 10 0 to 10 0 to 10
Description
Prescriptions—did you take them? Level of anger feelings
Level of anxious feelings
Level of sad feelings
SI
0 to 10 Yes or NO
Suicidal Ideation—Level of thoughts related to death. Were you planning? Did you act on those thoughts, urges, feelings?
SIB
0 to 10 Yes or NO
Self-Injurious Behavior—Level of thoughts/urges to hurt oneself. Did you take action and hurt yourself purposefully?
TIB
0 to 10 Yes or NO
Therapy Interfering Behavior—Level of thoughts/urges.
Did you do anything that would get in the way of your therapy? (see TIB handout for examples)
Hrs of
Sleep Energy
Targets BPE
Number of Hours
0 to 10
#/10 Yes or NO Yes or NO
Sleep—average hours of sleep. Was it solid or broken/interrupted?
Rate your energy level. 0-3=mild; 4-6=moderate; 7-10=high to manic
How many of your target behaviors did you complete?
Build Positive Experience. Did you do something enjoyable?
Did you meet your daily goal?
What skills helped you meet your goal? List feelings and emotions experienced. Share one positive thing.
Goals
met?
Skills List
Feelings List Highlights List
*You will have a difficult time succeeding in program if you are not honest with yourself and others. Remember that this is a safe environment.
19
