
Page 16 - Peter Williams Portfolio
P. 16
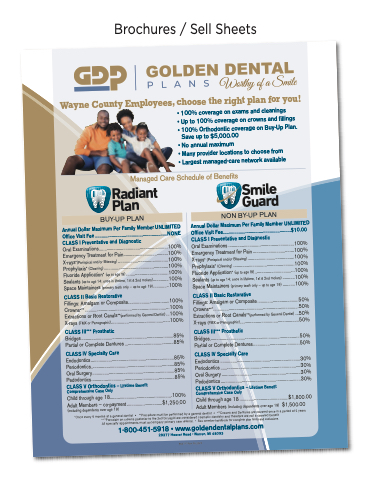
Brochures / Sell Sheets
Wayne County Employees, choose the right plan for you!
BUY-UP PLAN
NON BY-UP PLAN
Annual Dollar Maximum Per Family Member UNLIMITED Office Visit Fee .................................................................NONE CLASS I Preventative and Diagnostic
Oral Examinations..............................................................100% Emergency Treatment for Pain........................................100% X-rays*(Periapical and/or Bitewing) .............................................100% Prophylaxis* (Cleaning)..........................................................100% Fluoride Application* (up to age 19) ......................................100% Sealants (up to age 14; once in lifetime, 1st & 2nd molars)..............100% Space Maintainers (primary teeth only – up to age 19)..............100%
Annual Dollar Maximum Per Family Member UNLIMITED Office Visit Fee.............................................................$10.00 CLASS I Preventative and Diagnostic
Oral Examinations ...........................................................100% Emergency Treatment for Pain .....................................100% X-rays* (Periapical and/or Bitewing) ..........................................100% Prophylaxis* (Cleaning) .......................................................100% Fluoride Application* (up to age19)....................................100% Sealants (up to age 14; once in lifetime, 1st & 2nd molars) ...........100% Space Maintainers (primary teeth only – up to age 19) ...........100%
CLASS II Basic Restorative
CLASS II Basic Restorative
• 100% coverage on exams and cleanings
• Up to 100% coverage on crowns and fillings
• 100% Orthodontic coverage on Buy-Up Plan. Save up to $5,000.00
• No annual maximum
• Many provider locations to choose from
• Largest managed-care network available
Managed Care Schedule of Benefits
Radiant
Smile
Plan
Guard
Fillings: Amalgam or Composite.....................................100% Crowns*** ............................................................................100% Extractions or Root Canals**(performed by General Dentist) ...100% X-rays (FMX or Panographic).....................................................100%
Fillings: Amalgam or Composite.....................................50% Crowns***.............................................................................50% Extractions or Root Canals**(performed by General Dentist) ...50% X-rays (FMX or Panographic).....................................................50%
CLASS III*** Prosthetic
CLASS III*** Prosthetic
Bridges ...................................................................................85% Partial or Complete Dentures ............................................85%
Bridges.................................................................................50% Partial or Complete Dentures..........................................50%
CLASS IV Specialty Care
CLASS IV Specialty Care
Endodontics...........................................................................85% Periodontics...........................................................................85% Oral Surgery..........................................................................85% Pedodontics...........................................................................85% CLASS V Orthodontics – Lifetime Benefit
Endodontics ........................................................................30% Periodontics ........................................................................30% Oral Surgery .......................................................................30% Pedodontics ........................................................................30% CLASS V Orthodontics – Lifetime Benefit
Comprehensive Case Only
Child through age 18........................................................100%
Comprehensive Case Only
Adult Members – co-payment ................................$1,250.00 (including dependents over age 19)
Child through age 18 ............................................$1,800.00 Adult Members (including dependents over age 19) $1,500.00
*Once every 6 months at a general dentist • **Procedure must be performed by a general dentist • ***Crowns and Dentures are covered once in a period of 5 years ****Porcelain on crowns posterior to the 2nd bicuspid are considered cosmetic dentistry and therefore are not a covered benefit
All specialty appointments must accompany primary care referral. • See member handbook for complete plan limits and exclusions.
1-800-451-5918 • www.goldendentalplans.com 29377 Hoover Road • Warren, MI 48093
8641 F Rev 05.2020
