
Page 10 - 2018 MDT Benefits & Notices
P. 10
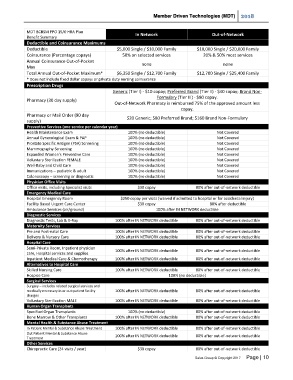
Member Driven Technologies (MDT) 2018
MDT BCBSM PPO 15/0 HRA Plan
Benefit Summary In Network Out-of-Network
Deductible and Coinsurance Maximums
Deductible $5,000 Single / $10,000 Family $10,000 Single / $20,000 Family
Coinsurance (Percentage copays) 50% on selected services 20% & 50% most services
Annual Coinsurance Out-of-Pocket none none
Max
Total Annual Out-of-Pocket Maximum* $6,350 Single / $12,700 Family $12,700 Single / $25,400 Family
* Does not include fixed dollar copays or private duty nursing coinsurance
Prescription Drugs
Generic (Tier I) - $10 copay; Preferred Brand (Tier II) - $40 copay; Brand Non-
Formulary (Tier III) - $80 copay.
Pharmacy (30 day supply)
Out-of-Network Pharmacy is reimbursed 75% of the approved amount less
copay.
Pharmacy or Mail Order (90 day
$20 Generic; $80 Preferred Brand; $160 Brand Non-Formulary
supply)
Preventive Services (one service per calendar year)
Health Maintenance Exam 100% (no deductible) Not Covered
Annual Gynecological Exam & PAP 100% (no deductible) Not Covered
Prostate Specific Antigen (PSA) Screening 100% (no deductible) Not Covered
Mammography Screening 100% (no deductible) Not Covered
Expanded Women’s Preventive Care 100% (no deductible) Not Covered
Voluntary Sterilization FEMALE 100% (no deductible) Not Covered
Well-Baby and Child Care 100% (no deductible) Not Covered
Immunizations – pediatric & adult 100% (no deductible) Not Covered
Colonoscopy – screening or diagnostic 100% (no deductible) Not Covered
Physician Office Visits
Office visits, including Specialist visits $30 copay 80% after out-of-network deductible
Emergency Medical Care
Hospital Emergency Room $250 copay per visits (waived if admitted to hospital or for accidental injury)
Facility Based Urgent Care Center $30 copay 80% after deductible
Ambulance Services (air/ground) 100% after IN NETWORK deductible
Diagnostic Services
Diagnostic Tests, Lab & X-Ray 100% after IN NETWORK deductible 80% after out-of-network deductible
Maternity Services
Pre and Post-natal Care 100% after IN NETWORK deductible 80% after out-of-network deductible
Delivery & Nursery Care 100% after IN NETWORK deductible 80% after out-of-network deductible
Hospital Care
Semi-Private Room, Inpatient physician 100% after IN NETWORK deductible 80% after out-of-network deductible
care, Hospital services and supplies
Inpatient Medical Care & Chemotherapy 100% after IN NETWORK deductible 80% after out-of-network deductible
Alternatives to Hospital Care
Skilled Nursing Care 100% after IN NETWORK deductible 80% after out-of-network deductible
Hospice Care 100% (no deductible)
Surgical Services
Surgery – includes related surgical services and
medically necessary in or out-patient facility 100% after IN NETWORK deductible 80% after out-of-network deductible
charges
Voluntary Sterilization MALE 100% after IN NETWORK deductible 80% after out-of-network deductible
Human Organ Transplants
Specified Organ Transplants 100% (no deductible) 80% after out-of-network deductible
Bone Marrow & Other Transplants 100% after IN NETWORK deductible 80% after out-of-network deductible
Mental Health & Substance Abuse Treatment
In Patient Mental & Substance Abuse Treatment 100% after IN NETWORK deductible 80% after out-of-network deductible
Out Patient Mental & Substance Abuse
Treatment 100% after IN NETWORK deductible 80% after out-of-network deductible
Other Services
Chiropractic Care (24 visits / year) $30 copay 80% after out-of-network deductible
Salus Group © Copyright 2017 Page | 10