
Page 64 - Avatar 2022 Flipbook
P. 64
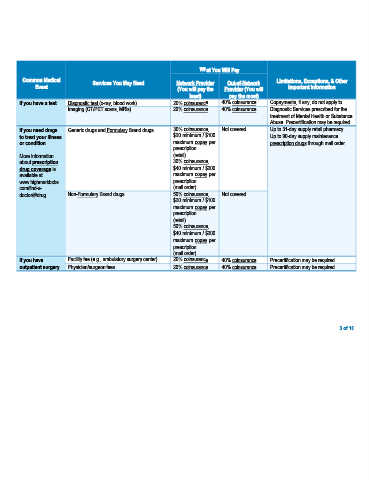
What You Will Pay
Common Medical Services You May Need Network Provider Out-of-Network Limitations, Exceptions, & Other
Event (You will pay the Provider (You will Important Information
least) pay the most)
If you have a test Diagnostic test (x-ray, blood work) 20% coinsurance 40% coinsurance Copayments, if any, do not apply to
Imaging (CT/PET scans, MRIs) 20% coinsurance 40% coinsurance Diagnostic Services prescribed for the
treatment of Mental Health or Substance
Abuse. Precertification may be required.
If you need drugs Generic drugs and Formulary Brand drugs 30% coinsurance, Not covered Up to 31-day supply retail pharmacy.
to treat your illness $20 minimum / $100 Up to 90-day supply maintenance
or condition maximum copay per prescription drugs through mail order.
prescription
More information (retail)
about prescription 30% coinsurance,
drug coverage is $40 minimum / $200
available at maximum copay per
www.highmarkbcbs. prescription
com/find-a- (mail order)
doctor/#/drug. Non-Formulary Brand drugs 50% coinsurance, Not covered
$20 minimum / $100
maximum copay per
prescription
(retail)
50% coinsurance,
$40 minimum / $200
maximum copay per
prescription
(mail order)
If you have Facility fee (e.g., ambulatory surgery center) 20% coinsurance 40% coinsurance Precertification may be required.
outpatient surgery Physician/surgeon fees 20% coinsurance 40% coinsurance Precertification may be required.
3 of 10