
Page 7 - Impact XM 2023 Benefit Guide
P. 7
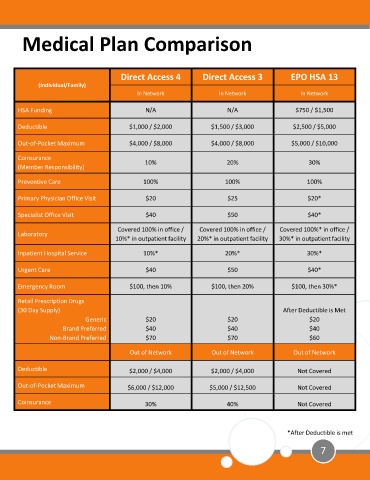
Medical Plan Comparison
Direct Access 4 Direct Access 3 EPO HSA 13
(Individual/Family)
In Network In Network In Network
HSA Funding N/A N/A $750 / $1,500
Deductible $1,000 / $2,000 $1,500 / $3,000 $2,500 / $5,000
Out-of-Pocket Maximum $4,000 / $8,000 $4,000 / $8,000 $5,000 / $10,000
Coinsurance
10% 20% 30%
(Member Responsibility)
Preventive Care 100% 100% 100%
Primary Physician Office Visit $20 $25 $20*
Specialist Office Visit $40 $50 $40*
Covered 100% in office / Covered 100% in office / Covered 100%* in office /
Laboratory
10%* in outpatient facility 20%* in outpatient facility 30%* in outpatient facility
Inpatient Hospital Service 10%* 20%* 30%*
Urgent Care $40 $50 $40*
Emergency Room $100, then 10% $100, then 20% $100, then 30%*
Retail Prescription Drugs
(30 Day Supply) After Deductible is Met
Generic $20 $20 $20
Brand Preferred $40 $40 $40
Non-Brand Preferred $70 $70 $60
Out of Network Out of Network Out of Network
Deductible $2,000 / $4,000 $2,000 / $4,000 Not Covered
Out-of-Pocket Maximum $6,000 / $12,000 $5,000 / $12,500 Not Covered
Coinsurance 30% 40% Not Covered
*After Deductible is met
7