
Page 12 - PetVet 2022 Master Benefits Guide_FINAL Version
P. 12
Dental
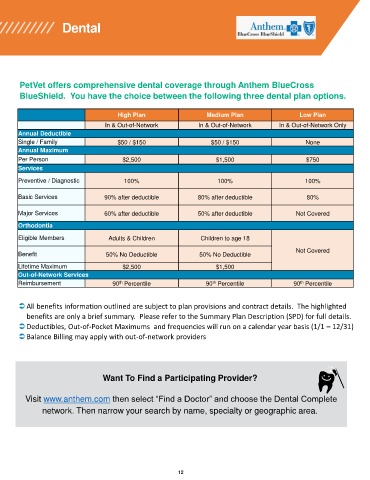
PetVet offers comprehensive dental coverage through Anthem BlueCross
BlueShield. You have the choice between the following three dental plan options.
High Plan Medium Plan Low Plan
In & Out-of-Network In & Out-of-Network In & Out-of-Network Only
Annual Deductible
Single / Family $50 / $150 $50 / $150 None
Annual Maximum
Per Person $2,500 $1,500 $750
Services
Preventive / Diagnostic 100% 100% 100%
Basic Services 90% after deductible 80% after deductible 80%
Major Services 60% after deductible 50% after deductible Not Covered
Orthodontia
Eligible Members Adults & Children Children to age 18
Not Covered
Benefit 50% No Deductible 50% No Deductible
Lifetime Maximum $2,500 $1,500
Out-of-Network Services
th
Reimbursement 90 Percentile 90 Percentile 90 Percentile
th
th
All benefits information outlined are subject to plan provisions and contract details. The highlighted
benefits are only a brief summary. Please refer to the Summary Plan Description (SPD) for full details.
Deductibles, Out-of-Pocket Maximums and frequencies will run on a calendar year basis (1/1 – 12/31)
Balance Billing may apply with out-of-network providers
Want To Find a Participating Provider?
Visit www.anthem.com then select “Find a Doctor” and choose the Dental Complete
network. Then narrow your search by name, specialty or geographic area.
12