
Page 79 - 2022 Washington Nationals Flipbook
P. 79
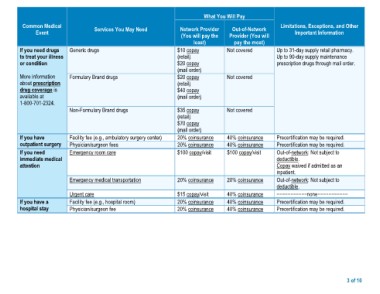
What You Will Pay
Common Medical Services You May Need Network Provider Out-of-Network Limitations, Exceptions, and Other
Event (You will pay the Provider (You will Important Information
If you need drugs Generic drugs least) pay the most) Up to 31-day supply retail pharmacy.
to treat your illness Not covered Up to 90-day supply maintenance
or condition $10 copay prescription drugs through mail order.
(retail) Not covered
More information Formulary Brand drugs $20 copay
about prescription Non-Formulary Brand drugs (mail order)
drug coverage is
$20 copay
available at (retail)
1-800-701-2324. $40 copay
(mail order)
If you have Facility fee (e.g., ambulatory surgery center) $35 copay Not covered Precertification may be required.
outpatient surgery Physician/surgeon fees (retail) Precertification may be required.
$70 copay 40% coinsurance
If you need Emergency room care (mail order) 40% coinsurance Out-of-network: Not subject to
immediate medical 20% coinsurance $100 copay/visit deductible.
attention 20% coinsurance Copay waived if admitted as an
$100 copay/visit 20% coinsurance inpatient.
Emergency medical transportation 40% coinsurance
20% coinsurance 40% coinsurance Out-of-network: Not subject to
If you have a Urgent care 40% coinsurance deductible.
hospital stay $15 copay/visit
Facility fee (e.g., hospital room) 20% coinsurance −−−−−−−−−−−none−−−−−−−−−−−
Physician/surgeon fee 20% coinsurance
Precertification may be required.
Precertification may be required.
3 of 10