
Page 11 - Avatar 2022 Flipbook
P. 11
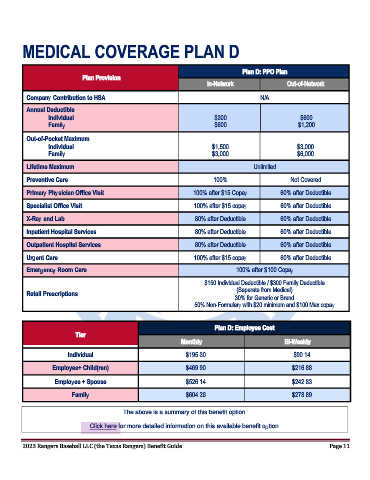
MEDICAL COVERAGE PLAN D
Plan D: PPO Plan
Plan Provision
In-Network Out-of-Network
Company Contribution to HSA N/A
Annual Deductible
Individual $300 $600
Family $600 $1,200
Out-of-Pocket Maximum
Individual $1,500 $3,000
Family $3,000 $6,000
Lifetime Maximum Unlimited
Preventive Care 100% Not Covered
Primary Physician Office Visit 100% after $15 Copay 60% after Deductible
Specialist Office Visit 100% after $15 copay 60% after Deductible
X-Ray and Lab 80% after Deductible 60% after Deductible
Inpatient Hospital Services 80% after Deductible 60% after Deductible
Outpatient Hospital Services 80% after Deductible 60% after Deductible
Urgent Care 100% after $15 copay 60% after Deductible
Emergency Room Care 100% after $100 Copay
$150 Individual Deductible / $300 Family Deductible
(Separate from Medical)
Retail Prescriptions
30% for Generic or Brand
50% Non-Formulary with $20 minimum and $100 Max copay
Plan D: Employee Cost
Tier
Monthly Bi-Weekly
Individual $195.30 $90.14
Employee+ Child(ren) $469.90 $216.88
Employee + Spouse $526.14 $242.83
Family $604.26 $278.89
The above is a summary of this benefit option.
Click here for more detailed information on this available benefit option.
2023 Rangers Baseball LLC (the Texas Rangers) Benefit Guide Page 11