
Page 7 - 2022 Local 502 Mersen Benefit Guide
P. 7
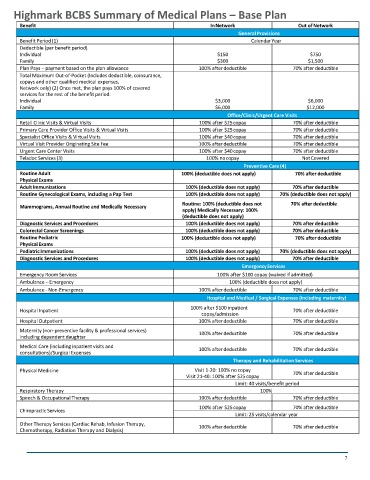
Highmark BCBS Summary of Medical Plans – Base Plan
Benefit In Network Out of Network
General Provisions
Benefit Period (1) Calendar Year
Deductible (per benefit period)
Individual $150 $750
Family $300 $1,500
Plan Pays – payment based on the plan allowance
70% after deductible
Benefit 100% after deductible Out of Network
In Network
Total Maximum Out-of-Pocket (Includes deductible, coinsurance,
copays and other qualified medical expenses, General Provisions
Network only) (2) Once met, the plan pays 100% of covered
Benefit Period (1) Calendar Year
services for the rest of the benefit period.
Individual $3,000 $6,000
Deductible (per benefit period) $6,000 $12,000
Family
Office/Clinic/Urgent Care Visits
$150
Individual 100% after $25 copay 70% after deductible
$750
Retail Clinic Visits & Virtual Visits
$300
$1,500
Family 100% after $25 copay 70% after deductible
Primary Care Provider Office Visits & Virtual Visits
Specialist Office Visits & Virtual Visits 100% after $40 copay 70% after deductible
Plan Pays – payment based on the plan allowance 100% after deductible 70% after deductible
100% after deductible
Virtual Visit Provider Originating Site Fee
70% after deductible
Urgent Care Center Visits 100% after $40 copay 70% after deductible
Total Maximum Out-of-Pocket (Includes deductible, coinsurance, 100% no copay Not Covered
Teladoc Services (3)
copays and other qualified medical expenses,
Preventive Care (4)
Routine Adult
Network only) (2) Once met, the plan pays 100% of covered 100% (deductible does not apply) 70% after deductible
services for the rest of the benefit period.
Physical Exams
70% after deductible
Adult Immunizations
$6,000
$3,000
Individual 100% (deductible does not apply) 70% (deductible does not apply)
100% (deductible does not apply)
Routine Gynecological Exams, including a Pap Test
$6,000
Family Routine: 100% (deductible does not 70% after de
$12,000 ductible
Mammograms, Annual Routine and Medically Necessary apply) Medically Necessary: 100%
Office/Clinic/Urgent Care Visits
(deductible does not apply)
70% after deductible
Diagnostic Services and Procedures
Retail Clinic Visits & Virtual Visits 100% (deductible does not apply) 70% after deductible
100% after $25 copay
70% after deductible
100% (deductible does not apply)
Colorectal Cancer Screenings
100% after $25 copay
Primary Care Provider Office Visits & Virtual Visits 100% (deductible does not apply) 70% after deductible
Routine Pediatric
70% after deductible
Physical Exams
70% after deductible
Specialist Office Visits & Virtual Visits 100% (deductible does not apply) 70% (deductible does not apply)
100% after $40 copay
Pediatric Immunizations
Diagnostic Services and Procedures 100% (deductible does not apply) 70% after deductible
Virtual Visit Provider Originating Site Fee 100% after deductible Emergency Services 70% after deductible
Urgent Care Center Visits 100% after $40 copay 70% after deductible
Emergency Room Services
100% after $100 copay (waived if admitted)
Ambulance – Emergency 100% (deductible does not apply)
Teladoc Services (3) 100% no copay 70% after deductible
Not Covered
Ambulance - Non-Emergency
100% after deductible
Preventive Care (4) Hospital and Medical / Surgical Expenses (including maternity)
100% after $100 inpatient
Hospital Inpatient
70% after deductible
Routine Adult 100% (deductible does not apply) 70% after deductible
copay/admission
Hospital Outpatient
Physical Exams 100% after deductible 70% after deductible
Maternity (non-preventive facility & professional services)
Adult Immunizations 100% (deductible does not apply) 70% after deductible
70% after deductible
100% after deductible
including dependent daughter
Routine Gynecological Exams, including a Pap Test 100% (deductible does not apply) 70% (deductible does not apply)
Medical Care (including inpatient visits and
100% after deductible
70% after deductible
consultations)/Surgical Expenses
Therapy and Rehabilitation Services
Mammograms, Annual Routine and Medically Necessary Routine: 100% (deductible does not apply) Medically
Physical Medicine Necessary: 100% (deductible does not apply) 70% after deductible
Visit 1-20: 100% no copay
Visit 21-40: 100% after $25 copay
Diagnostic Services and Procedures 100% (deductible does not apply) 70% after deductible
Limit: 40 visits/benefit period
Colorectal Cancer Screenings 100% (deductible does not apply) 100% 70% after deductible
Respiratory Therapy
Speech & Occupational Therapy 100% after deductible 70% after deductible
Routine Pediatric 100% (deductible does not apply) 70% after deductible
Chiropractic Services 100% after $25 copay 70% after deductible
Physical Exams Limit: 25 visits/calendar year
Other Therapy Services (Cardiac Rehab, Infusion Therapy,
Pediatric Immunizations 100% (deductible does not apply) 70% (deductible does not apply)
70% after deductible
100% after deductible
Chemotherapy, Radiation Therapy and Dialysis)
Diagnostic Services and Procedures 100% (deductible does not apply) 70% after deductible
Emergency Services
7
Emergency Room Services 100% after $100 copay (waived if admitted)
Ambulance – Emergency 100% (deductible does not apply)