
Page 36 - 2021 Dreyer's New Hire Guide
P. 36
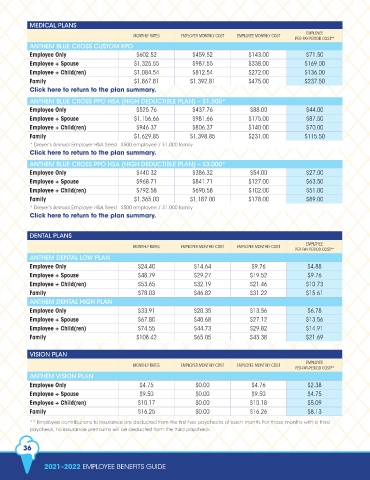
MEDICAL PLANS
EMPLOYEE
MONTHLY RATES EMPLOYER MONTHLY COST EMPLOYEE MONTHLY COST
PER-PAY-PERIOD COST**
ANTHEM BLUE CROSS CUSTOM EPO
Employee Only $602.52 $459.52 $143.00 $71.50
Employee + Spouse $1,325.55 $987.55 $338.00 $169.00
Employee + Child(ren) $1,084.54 $812.54 $272.00 $136.00
Family $1,867.81 $1,392.81 $475.00 $237.50
Click here to return to the plan summary.
ANTHEM BLUE CROSS PPO HSA (HIGH DEDUCTIBLE PLAN) – $1,500*
Employee Only $525.76 $437.76 $88.00 $44.00
Employee + Spouse $1,156.66 $981.66 $175.00 $87.50
Employee + Child(ren) $946.37 $806.37 $140.00 $70.00
Family $1,629.85 $1,398.85 $231.00 $115.50
* Dreyer’s Annual Employer HSA Seed: $500 employee / $1,000 family
Click here to return to the plan summary.
ANTHEM BLUE CROSS PPO HSA (HIGH DEDUCTIBLE PLAN) – $3,000*
Employee Only $440.32 $386.32 $54.00 $27.00
Employee + Spouse $968.71 $841.71 $127.00 $63.50
Employee + Child(ren) $792.58 $690.58 $102.00 $51.00
Family $1,365.00 $1,187.00 $178.00 $89.00
* Dreyer’s Annual Employer HSA Seed: $500 employee / $1,000 family
Click here to return to the plan summary.
DENTAL PLANS
EMPLOYEE
MONTHLY RATES EMPLOYER MONTHLY COST EMPLOYEE MONTHLY COST
PER-PAY-PERIOD COST**
ANTHEM DENTAL LOW PLAN
Employee Only $24.40 $14.64 $9.76 $4.88
Employee + Spouse $48.79 $29.27 $19.52 $9.76
Employee + Child(ren) $53.65 $32.19 $21.46 $10.73
Family $78.03 $46.82 $31.22 $15.61
ANTHEM DENTAL HIGH PLAN
Employee Only $33.91 $20.35 $13.56 $6.78
Employee + Spouse $67.80 $40.68 $27.12 $13.56
Employee + Child(ren) $74.55 $44.73 $29.82 $14.91
Family $108.42 $65.05 $43.38 $21.69
VISION PLAN
EMPLOYEE
MONTHLY RATES EMPLOYER MONTHLY COST EMPLOYEE MONTHLY COST
PER-PAY-PERIOD COST**
ANTHEM VISION PLAN
Employee Only $4.75 $0.00 $4.76 $2.38
Employee + Spouse $9.50 $0.00 $9.50 $4.75
Employee + Child(ren) $10.17 $0.00 $10.18 $5.09
Family $16.25 $0.00 $16.26 $8.13
** Employee contributions to insurance are deducted from the first two paychecks of each month. For those months with a third
paycheck, no insurance premiums will be deducted from the third paycheck.
36
2021–2022 EMPLOYEE BENEFITS GUIDE