
Page 11 - 2022 Mersen Benefit Guide
P. 11
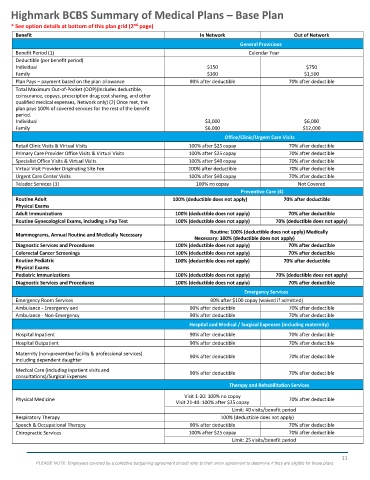
Highmark BCBS Summary of Medical Plans – Base Plan
nd
* See o ption details at bottom of this plan grid (2 page)
Benefit In Network Out of Network
During 2023 open enrollment, the Base Plan will only be available to active employees that selected this plan for the 2022 benefit
General Provisions
plan year. Calendar Year
Benefit Period (1)
Deductible (per benefit period) $150 $750
Individual
Family $300 $1,500
Plan Pays – payment based on the plan allowance 90% after deductible 70% after deductible
Total Maximum Out-of-Pocket (OOP)(Includes deductible,
coinsurance, copays, prescription drug cost sharing, and other
qualified medical expenses, Network only) (2) Once met, the
plan pays 100% of covered services for the rest of the benefit
period.
Individual $3,000 $6,000
Family $6,000 $12,000
Office/Clinic/Urgent Care Visits
Retail Clinic Visits & Virtual Visits 100% after $25 copay 70% after deductible
Primary Care Provider Office Visits & Virtual Visits 100% after $25 copay 70% after deductible
Specialist Office Visits & Virtual Visits 100% after $40 copay 70% after deductible
Virtual Visit Provider Originating Site Fee 100% after deductible 70% after deductible
Urgent Care Center Visits 100% after $40 copay 70% after deductible
Teladoc Services (3) 100% no copay Not Covered
Preventive Care (4)
Routine Adult 100% (deductible does not apply) 70% after deductible
Physical Exams
Adult Immunizations 100% (deductible does not apply) 70% after deductible
Routine Gynecological Exams, including a Pap Test 100% (deductible does not apply) 70% (deductible does not apply)
Routine: 100% (deductible does not apply) Medically
Mammograms, Annual Routine and Medically Necessary
Necessary: 100% (deductible does not apply)
Diagnostic Services and Procedures 100% (deductible does not apply) 70% after deductible
Colorectal Cancer Screenings 100% (deductible does not apply) 70% after deductible
Routine Pediatric 100% (deductible does not apply) 70% after deductible
Physical Exams
Pediatric Immunizations 100% (deductible does not apply) 70% (deductible does not apply)
Diagnostic Services and Procedures 100% (deductible does not apply) 70% after deductible
Emergency Services
Emergency Room Services 90% after $100 copay (waived if admitted)
Ambulance - Emergency and 90% after deductible 70% after deductible
Ambulance - Non-Emergency 90% after deductible 70% after deductible
Hospital and Medical / Surgical Expenses (including maternity)
Hospital Inpatient 90% after deductible 70% after deductible
Hospital Outpatient 90% after deductible 70% after deductible
Maternity (non-preventive facility & professional services) 90% after deductible 70% after deductible
including dependent daughter
Medical Care (including inpatient visits and 90% after deductible 70% after deductible
consultations)/Surgical Expenses
Therapy and Rehabilitation Services
Visit 1-20: 100% no copay
Physical Medicine 70% after deductible
Visit 21-40: 100% after $25 copay
Limit: 40 visits/benefit period
Respiratory Therapy 100% (deductible does not apply)
Speech & Occupational Therapy 90% after deductible 70% after deductible
Chiropractic Services 100% after $25 copay 70% after deductible
Limit: 25 visits/benefit period
11
PLEASE NOTE: Employees covered by a collective bargaining agreement should refer to their union agreement to determine if they are eligible for these plans.