
Page 66 - RADC Bulletin 2021
P. 66
Very High Risk Recruits at Pirbright
Lt Col A Davis
The Coronavirus (C19) pandemic continues to have far-reaching impacts across the world and within Primary Dental Care.
At the Army Training Centre Pirbright (ATC(P)), and across Phase 1, recruiting was paused from March 2020 - Jun 2020, with medical assessments for new recruits being impacted, delayed and deferred.
The impact on the entire 14-week initial training programme was also stark with this being condensed to 12 weeks, strict bubble protocols enforced, frequent periods of isolation for 12-person sections suspected of C19 and access to recruits for dental
care being severely limited. Normal training has resumed but in order to address the recruitment pause and impact of C19, Phase 1 intakes are now aggressively loaded with an unrelenting pace for all involved, with high intake numbers in place but access issues still present and enduring.
To ensure appropriate fitness standards prior to enlisting, all potential recruits should undergo a physical assessment including
a basic oral examination by doctors employed by Capita at the four Assessment Centres in Belfast, Edinburgh, Lichfield
and Pirbright. The Pre-Entry medical was modified by Capita to reflect the impact
and risk of C19 resulting in cessation of the oral examination. Awareness of the Pre- Entry Oral and Maxillofacial Policy (JSP 950 6-7-7 4-M-1 - Joint Medical Employment Standards) outlines a definition for doctors to identify and reject candidates with gross oral neglect, ‘multiple open carious cavities’ alongside other reasons to be deemed Unfit to enlist.
A prospective audit of 100 recruits at IDI assessed Category, Treatment Need (TN) and whether or not they had received an intra-oral examination at their Assessment Centre. This showed that 5% of recruits failed to meet the policy standards but
had received a Pre-Entry oral exam demonstrating failure to correctly implement the policy. There is no Chain of Command appetite to reject these recruits at IDI when dentist-diagnosed oral neglect is evident. Efforts are ongoing to offer initial support and advice to Capita to be able to properly
Table 1. Retrospective audit into IDI fitness data.
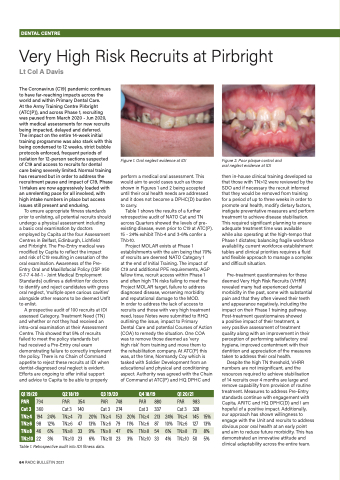
Figure 1. Oral neglect evidence at IDI
perform a medical oral assessment. This would aim to avoid cases such as those shown in Figures 1 and 2 being accepted until their oral health needs are addressed and it does not become a DPHC(D) burden to carry.
Table 1 shows the results of a further retrospective audit of NATO Cat and TN across Quarters showed the levels of pre- existing disease, even prior to C19 at ATC(P). 15 - 24% exhibit TN>4 and 3-6% confer a TN>10.
Project MOLAR exists at Phase 1 establishments with the aim being that 70% of recruits are deemed NATO Category 1
at the end of Initial Training. The impact of C19 and additional PPE requirements, AGP fallow time, recruit access within Phase 1 and often high TN risks failing to meet the Project MOLAR target, failure to address diagnosed disease, worsening morbidity and reputational damage to the MOD.
In order to address the lack of access to recruits and those with very high treatment need, Issue Notes were submitted to RHQ outlining the issue, impact to Primary Dental Care and potential Courses of Action (COA) to remedy the situation. One COA was to remove those deemed as ‘very
high risk’ from training and move them to the rehabilitation company. At ATC(P) this was, at the time, Normandy Coy which is tasked with Soldier Development from an educational and physical and conditioning aspect. Authority was agreed with the Chain of Command at ATC(P) and HQ DPHC and
Figure 2. Poor plaque control and oral neglect evidence at IDI
then in-house clinical training developed so that those with TN>12 were reviewed by the SDO and if necessary the recruit informed that they would be removed from training for a period of up to three weeks in order to promote oral health, modify dietary factors, instigate preventative measures and perform treatment to achieve disease stabilisation. This required significant planning to ensure adequate treatment time was available
while also operating at the high-tempo that Phase 1 dictates; balancing fragile workforce availability, current workforce establishment tables and clinical priorities requires a fluid and flexible approach to manage a complex and difficult situation.
Pre-treatment questionnaires for those deemed Very High Risk Recruits (VHRR) revealed many had experienced dental morbidity in the past, some with substantial pain and that they often viewed their teeth and appearance negatively, including the impact on their Phase 1 training pathway. Post-treatment questionnaires showed
a positive impact of their treatment, a
very positive assessment of treatment quality along with an improvement in their perception of performing satisfactory oral hygiene, improved contentment with their dentition and appreciation of the measures taken to address their oral health.
Despite the high TN threshold, VHRR numbers are not insignificant, and the resources required to achieve stabilisation of 14 recruits over 4 months are large and remove capability from provision of routine treatment. Measures to address Pre-Entry standards continue with engagement with Capita, ARITC and HQ DPHC(D) and I am hopeful of a positive impact. Additionally, our approach has shown willingness to engage with the Unit and recruits to address obvious poor oral health at an early point and aim to reduce future morbidity. This has demonstrated an innovative attitude and clinical adaptability across the entire team.
Q1 19/20
Q2 18/19
Q3 19/20
Q4 18/19
Q1 20/21
PAR
794
PAR
354
PAR
748
PAR
880
PAR
983
Cat 3
360
Cat 3
140
Cat 3
274
Cat 3
337
Cat 3
328
TN≥4
194
24%
TN≥4
70
20%
TN≥4
153
20%
TN≥4
213
24%
TN≥4
145
15%
TN≥6
98
12%
TN≥6
47
13%
TN≥6
79
11%
TN≥6
87
10%
TN≥6
127
13%
TN≥8
46
6%
TN≥8
33
9%
TN≥8
47
6%
TN≥8
54
6%
TN≥8
79
8%
TN≥10
22
3%
TN≥10
23
6%
TN≥10
23
3%
TN≥10
33
4%
TN≥10
50
5%
64 RADC BULLETIN 2021
DENTAL CENTRE
