
Page 10 - 2023-24 Gas Clip Technologies Benefit Guide EXECUTIVES
P. 10
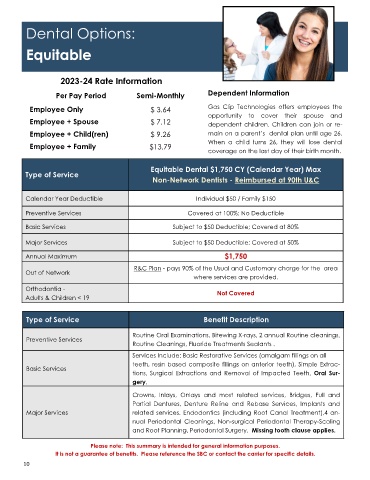
Dental Options:
Equitable
2023-24 Rate Information
Per Pay Period Semi-Monthly Dependent Information
Employee Only $ 3.64 Gas Clip Technologies offers employees the
opportunity to cover their spouse and
Employee + Spouse $ 7.12 dependent children. Children can join or re-
Employee + Child(ren) $ 9.26 main on a parent’s dental plan until age 26.
When a child turns 26, they will lose dental
Employee + Family $13.79
coverage on the last day of their birth month.
Equitable Dental $1,750 CY (Calendar Year) Max
Type of Service
Non-Network Dentists - Reimbursed at 90th U&C
Calendar Year Deductible Individual $50 / Family $150
Preventive Services Covered at 100%; No Deductible
Basic Services Subject to $50 Deductible; Covered at 80%
Major Services Subject to $50 Deductible; Covered at 50%
Annual Maximum $1,750
R&C Plan - pays 90% of the Usual and Customary charge for the area
Out of Network
where services are provided.
Orthodontia - Not Covered
Adults & Children < 19
Type of Service Benefit Description
Routine Oral Examinations, Bitewing X-rays, 2 annual Routine cleanings,
Preventive Services
Routine Cleanings, Fluoride Treatments Sealants .
Services Include: Basic Restorative Services (amalgam fillings on all
teeth, resin based composite fillings on anterior teeth), Simple Extrac-
Basic Services
tions, Surgical Extractions and Removal of Impacted Teeth, Oral Sur-
gery,
Crowns, Inlays, Onlays and most related services, Bridges, Full and
Partial Dentures, Denture Reline and Rebase Services, Implants and
Major Services related services. Endodontics (including Root Canal Treatment),4 an-
nual Periodontal Cleanings, Non-surgical Periodontal Therapy-Scaling
and Root Planning, Periodontal Surgery. Missing tooth clause applies.
Please note: This summary is intended for general information purposes.
It is not a guarantee of benefits. Please reference the SBC or contact the carrier for specific details.
10