
Page 4 - IFC Roofing Benefit Guide 2-1-22
P. 4
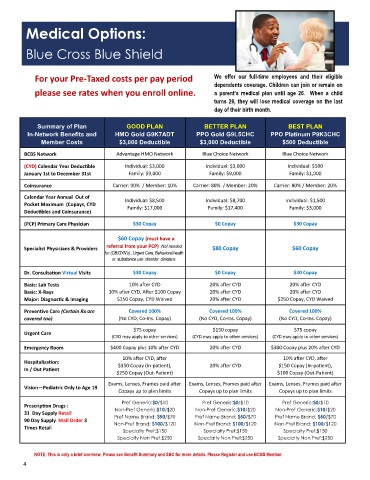
Medical Options:
Blue Cross Blue Shield
For your Pre-Taxed costs per pay period We offer our full-time employees and their eligible
dependents coverage. Children can join or remain on
please see rates when you enroll online. a parent’s medical plan until age 26. When a child
turns 26, they will lose medical coverage on the last
day of their birth month.
Summary of Plan OD PLAN BETTER PLAN BEST PLAN
O
G
In-Network Benefits and HMO Gold G9K7ADT PPO Gold G9L5CHC PPO Platinum P9K3CHC
Member Costs $3,000 Deductible $3,000 Deductible $500 Deductible
BCBS Network Advantage HMO Network Blue Choice Network Blue Choice Network
(CYD) Calendar Year Deductible Individual: $3,000 Individual: $3,000 Individual: $500
January 1st to December 31st Family: $9,000 Family: $9,000 Family: $1,000
Coinsurance Carrier: 90% / Member: 10% Carrier: 80% / Member: 20% Carrier: 80% / Member: 20%
Calendar Year Annual Out of
Individual: $8,500 Individual: $8,700 Individual: $1,500
Pocket Maximum (Copays, CYD
Family: $17,000 Family: $17,400 Family: $3,000
Deductibles and Coinsurance)
(PCP) Primary Care Physician $30 Copay $0 Copay $30 Copay
$60 Copay (must have a
referral from your PCP) Not needed
Specialist Physicians & Providers $80 Copay $60 Copay
for (OB/GYN’s)., Urgent Care, Behavioral health
or use disorder clinicians.
Dr. Consultation Virtual Visits $30 Copay $0 Copay $30 Copay
Basic: Lab Tests 10% after CYD 20% after CYD 20% after CYD
Basic: X-Rays 10% after CYD, After $100 Copay 20% after CYD 20% after CYD
Major: Diagnostic & Imaging $250 Copay, CYD Waived 20% after CYD $250 Copay, CYD Waived
C
o
C
o
v
v
Preventive Care (Certain Rx are Covered 100% ered 100% ered 100%
covered too) (No CYD, Co-Ins. Copay) (No CYD, Co-Ins. Copay) (No CYD, Co-Ins. Copay)
$75 copay $150 copay $75 copay
Urgent Care
(CYD may apply to other services) (CYD may apply to other services) (CYD may apply to other services)
Emergency Room $400 Copay plus 10% after CYD 20% after CYD $300 Copay plus 20% after CYD
10% after CYD, after 10% after CYD, after
Hospitalization:
$350 Copay (In-patient), 20% after CYD $150 Copay (In-patient),
In / Out Patient
$250 Copay (Out-Patient) $100 Copay (Out-Patient)
Exams, Lenses, Frames paid after Exams, Lenses, Frames paid after Exams, Lenses, Frames paid after
Vision—Pediatric Only to Age 19
Copays up to plan limits Copays up to plan limits Copays up to plan limits
Pref Generic:$0/$10 Pref Generic:$0/$10 Pref Generic:$0/$10
Prescription Drugs :
Non-Pref Generic:$10/$20 Non-Pref Generic:$10/$20 Non-Pref Generic:$10/$20
31 Day Supply Retail
Pref Name Brand: $50/$70 Pref Name Brand: $50/$70 Pref Name Brand: $50/$70
90 Day Supply Mail Order 3
Non-Pref Brand: $100/$120 Non-Pref Brand: $100/$120 Non-Pref Brand: $100/$120
Times Retail Specialty Pref:$150 Specialty Pref:$150 Specialty Pref:$150
Specialty Non Pref:$250 Specialty Non Pref:$250 Specialty Non Pref:$250
NOTE: This is only a brief overview. Please see Benefit Summary and SBC for more details. Please Register and use BCBS Member
4