
Page 18 - Megatel Homes LLC Benefit Guide 8-1-2025v3
P. 18
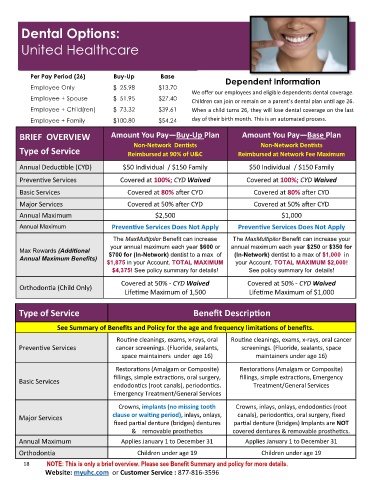
Dental Options:
United Healthcare
Per Pay Period (26) Buy-Up Base Dependent Information
Employee Only $ 25.98 $13.70
We offer our employees and eligible dependents dental coverage.
Employee + Spouse $ 51.95 $27.40
Children can join or remain on a parent’s dental plan until age 26.
Employee + Child(ren) $ 73.32 $39.61 When a child turns 26, they will lose dental coverage on the last
Employee + Family $100.80 $54.24 day of their birth month. This is an automated process.
BRIEF OVERVIEW Amount You Pay—Buy-Up Plan Amount You Pay—Base Plan
Non-Network Dentists Non-Network Dentists
Type of Service Reimbursed at 90% of U&C Reimbursed at Network Fee Maximum
Annual Deductible (CYD) $50 Individual / $150 Family $50 Individual / $150 Family
Preventive Services Covered at 100%; CYD Waived Covered at 100%; CYD Waived
Basic Services Covered at 80% after CYD Covered at 80% after CYD
Major Services Covered at 50% after CYD Covered at 50% after CYD
Annual Maximum $2,500 $1,000
Annual Maximum Preventive Services Does Not Apply Preventive Services Does Not Apply
The MaxMultipiler Benefit can increase The MaxMultipiler Benefit can increase your
your annual maximum each year $600 or annual maximum each year $250 or $350 for
Max Rewards (Additional
Annual Maximum Benefits) $700 for (In-Network) dentist to a max of (In-Network) dentist to a max of $1,000 in
$1,875 in your Account. TOTAL MAXIMUM your Account. TOTAL MAXIMUM $2,000!
$4,375! See policy summary for details! See policy summary for details!
Covered at 50% - CYD Waived Covered at 50% - CYD Waived
Orthodontia (Child Only)
Lifetime Maximum of 1,500 Lifetime Maximum of $1,000
Type of Service Benefit Description
See Summary of Benefits and Policy for the age and frequency limitations of benefits.
Routine cleanings, exams, x-rays, oral Routine cleanings, exams, x-rays, oral cancer
Preventive Services cancer screenings. (Fluoride, sealants, screenings. (Fluoride, sealants, space
space maintainers under age 16) maintainers under age 16)
Restorations (Amalgam or Composite) Restorations (Amalgam or Composite)
fillings, simple extractions, oral surgery, fillings, simple extractions, Emergency
Basic Services
endodontics (root canals), periodontics. Treatment/General Services
Emergency Treatment/General Services
Crowns, implants (no missing tooth Crowns, inlays, onlays, endodontics (root
Major Services clause or waiting period), inlays, onlays, canals), periodontics, oral surgery, fixed
fixed partial denture (bridges) dentures partial denture (bridges) Implants are NOT
& removable prosthetics covered dentures & removable prosthetics.
Annual Maximum Applies January 1 to December 31 Applies January 1 to December 31
Orthodontia Children under age 19 Children under age 19
18 NOTE: This is only a brief overview. Please see Benefit Summary and policy for more details.
Website: myuhc.com or Customer Service : 877-816-3596