
Page 4 - Advanced Neuro Solutions 2021 Benefit Guide Draft
P. 4
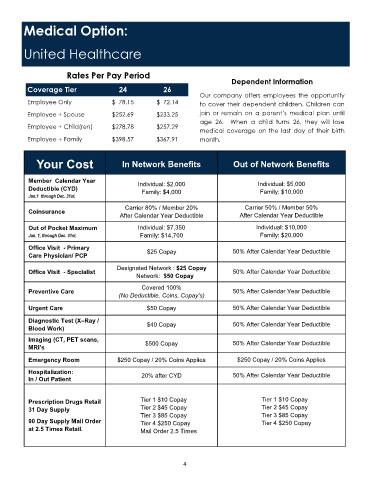
Medical Option:
United Healthcare
Rates Per Pay Period
Dependent Information
Coverage Tier 24 26
Our company offers employees the opportunity
Employee Only $ 78.15 $ 72.14 to cover their dependent children. Children can
Employee + Spouse $252.69 $233.25 join or remain on a parent’s medical plan until
age 26. When a child turns 26, they will lose
Employee + Child(ren) $278.78 $257.29
medical coverage on the last day of their birth
Employee + Family $398.57 $367.91 month.
Your Cost In Network Benefits Out of Network Benefits
Member Calendar Year Individual: $2,000 Individual: $5,000
Deductible (CYD) Family: $4,000 Family: $10,000
Jan.1 through Dec. 31st.
Carrier 80% / Member 20% Carrier 50% / Member 50%
Coinsurance
After Calendar Year Deductible After Calendar Year Deductible
Out of Pocket Maximum Individual: $7,350 Individual: $10,000
Jan. 1, through Dec. 31st. Family: $14,700 Family: $20,000
Office Visit - Primary 50% After Calendar Year Deductible
Care Physician/ PCP $25 Copay
Designated Network : $25 Copay
Office Visit - Specialist 50% After Calendar Year Deductible
Network: $50 Copay
Covered 100%
Preventive Care 50% After Calendar Year Deductible
(No Deductible, Coins, Copay’s)
Urgent Care $50 Copay 50% After Calendar Year Deductible
Diagnostic Test (X–Ray / $40 Copay 50% After Calendar Year Deductible
Blood Work)
Imaging (CT, PET scans, $500 Copay 50% After Calendar Year Deductible
MRI’s
Emergency Room $250 Copay / 20% Coins Applies $250 Copay / 20% Coins Applies
Hospitalization: 20% after CYD 50% After Calendar Year Deductible
In / Out Patient
Prescription Drugs Retail Tier 1 $10 Copay Tier 1 $10 Copay
31 Day Supply Tier 2 $45 Copay Tier 2 $45 Copay
Tier 3 $85 Copay Tier 3 $85 Copay
90 Day Supply Mail Order Tier 4 $250 Copay Tier 4 $250 Copay
at 2.5 Times Retail. Mail Order 2.5 Times
4