
Page 16 - Plainview Benefit Guide 4-1-24
P. 16
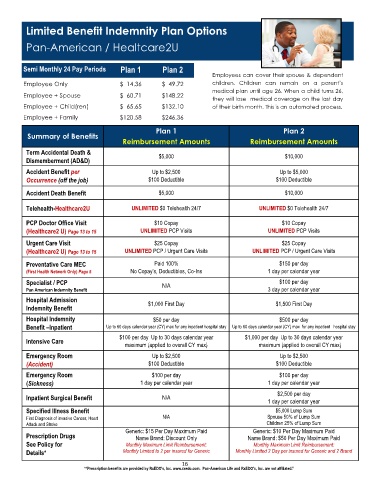
Limited Benefit Indemnity Plan Options
Pan-American / Healtcare2U
Semi Monthly 24 Pay Periods Plan 1 Plan 2
Employees can cover their spouse & dependent
Employee Only $ 14.36 $ 49.72 children. Children can remain on a parent’s
medical plan until age 26. When a child turns 26,
Employee + Spouse $ 60.71 $148.22
they will lose medical coverage on the last day
Employee + Child(ren) $ 65.65 $132.10 of their birth month. This is an automated process.
Employee + Family $120.58 $246.36
Plan 1 Plan 2
Summary of Benefits
Reimbursement Amounts Reimbursement Amounts
Term Accidental Death & $5,000 $10,000
Dismemberment (AD&D)
Accident Benefit per Up to $2,500 Up to $5,000
Occurrence (off the job) $100 Deductible $100 Deductible
Accident Death Benefit $5,000 $10,000
Telehealth-Healthcare2U UNLIMITED $0 Telehealth 24/7 UNLIMITED $0 Telehealth 24/7
PCP Doctor Office Visit $10 Copay $10 Copay
(Healthcare2 U) Page 13 to 15 UNLIMITED PCP Visits UNLIMITED PCP Visits
Urgent Care Visit $25 Copay $25 Copay
(Healthcare2 U) Page 13 to 15 UNLIMITED PCP / Urgent Care Visits UNLIMITED PCP / Urgent Care Visits
Preventative Care MEC Paid 100% $150 per day
(First Health Network Only) Page 5 No Copay’s, Deductibles, Co-Ins 1 day per calendar year
Specialist / PCP N/A $100 per day
Pan American Indemnity Benefit 3 day per calendar year
Hospital Admission $1,000 First Day $1,500 First Day
Indemnity Benefit
Hospital Indemnity $50 per day $500 per day
Benefit –Inpatient Up to 60 days calendar year (CY) max for any inpatient hospital stay Up to 60 days calendar year (CY) max for any inpatient hospital stay
$100 per day Up to 30 days calendar year $1,000 per day Up to 30 days calendar year
Intensive Care
maximum (applied to overall CY max) maximum (applied to overall CY max)
Emergency Room Up to $2,500 Up to $2,500
(Accident) $100 Deductible $100 Deductible
Emergency Room $100 per day $100 per day
(Sickness) 1 day per calendar year 1 day per calendar year
$2,500 per day
Inpatient Surgical Benefit N/A
1 day per calendar year
Specified Illness Benefit $5,000 Lump Sum
First Diagnosis of invasive Cancer, Heart N/A Spouse 50% of Lump Sum
Attack and Stroke Children 25% of Lump Sum
Generic: $15 Per Day Maximum Paid Generic: $10 Per Day Maximum Paid
Prescription Drugs Name Brand: Discount Only Name Brand: $50 Per Day Maximum Paid
See Policy for Monthly Maximum Limit Reimbursement: Monthly Maximum Limit Reimbursement:
Details* Monthly Limited to 2 per insured for Generic Monthly Limited 2 Day per insured for Generic and 2 Brand
16
*“Prescription benefits are provided by RxEDO's, Inc. www.rxedo.com. Pan-American Life and RxEDO's, Inc. are not affiliated.”