
Page 4 - Wesco Benefit Guide Effective 9-1-2020 Revised
P. 4
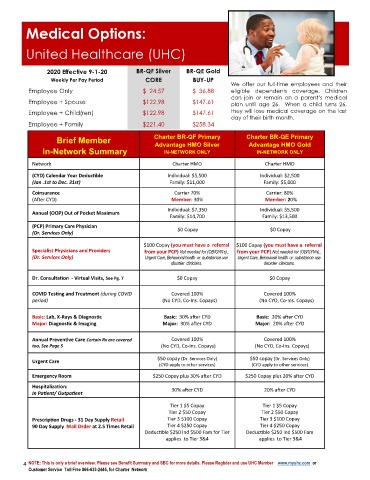
Medical Options:
United Healthcare (UHC)
2020 Effective 9-1-20 BR-QF Silver BR-QE Gold
Weekly Per Pay Period CORE BUY-UP
We offer our full-time employees and their
Employee Only $ 24.57 $ 36.88 eligible dependents coverage. Children
can join or remain on a parent’s medical
Employee + Spouse $122.98 $147.61 plan until age 26. When a child turns 26,
Employee + Child(ren) $122.98 $147.61 they will lose medical coverage on the last
day of their birth month.
Employee + Family $221.40 $258.34
Brief Member Charter BR-QF Primary Charter BR-QE Primary
Advantage HMO Silver
Advantage HMO Gold
In-Network Summary IN-NETWORK ONLY IN-NETWORK ONLY
Network Charter HMO Charter HMO
(CYD) Calendar Year Deductible Individual: $5,500 Individual: $2,500
(Jan .1st to Dec. 31st) Family: $11,000 Family: $5,000
Coinsurance Carrier 70% Carrier: 80%
(After CYD) Member: 30% Member: 20%
Individual: $7,350 Individual: $5,500
Annual (OOP) Out of Pocket Maximum
Family: $14,700 Family: $13,500
(PCP) Primary Care Physician
(Dr. Services Only) $0 Copay $0 Copay
$100 Copay (you must have a referral $100 Copay (you must have a referral
Specialist Physicians and Providers from your PCP) Not needed for (OB/GYN’s)., from your PCP) Not needed for (OB/GYN’s).,
(Dr. Services Only) Urgent Care, Behavioral health or use Urgent Care, Behavioral health or use
disorder clinicians. disorder clinicians.
Dr. Consultation - Virtual Visits, See Pg. 7 $0 Copay $0 Copay
COVID Testing and Treatment (during COVID Covered 100% Covered 100%
period) (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays)
Basic: Lab, X-Rays & Diagnostic Basic: 30% after CYD Basic: 20% after CYD
Major: Diagnostic & Imaging Major: 30% after CYD Major: 20% after CYD
Annual Preventive Care Certain Rx are covered Covered 100% Covered 100%
too, See Page 5 (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays)
$50 c
D
r
. S
o
p
(
ay
$50 copay (Dr. Services Only) ervices Only)
Urgent Care
(CYD apply to other services) (CYD apply to other services)
Emergency Room $250 Copay plus 30% after CYD $250 Copay plus 20% after CYD
Hospitalization:
30% after CYD 20% after CYD
In Patient/ Outpatient
Tier 1 $5 Copay Tier 1 $5 Copay
Tier 2 $50 Copay Tier 2 $50 Copay
Prescription Drugs - 31 Day Supply Retail Tier 3 $100 Copay Tier 3 $100 Copay
90 Day Supply Mail Order at 2.5 Times Retail Tier 4 $250 Copay Tier 4 $250 Copay
Deductible $250 Ind $500 Fam for Tier Deductible $250 Ind $500 Fam
applies to Tier 3&4 applies to Tier 3&4
4 NOTE: This is only a brief overview. Please see Benefit Summary and SBC for more details. Please Register and use UHC Member www.myuhc.com or
Customer Service Toll Free 866-633-2446, for Charter Network