
Page 4 - Megatel Homes LLC Benefit Guide 8-1-2025v2
P. 4
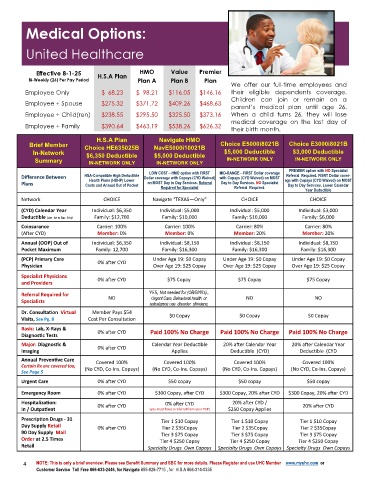
Medical Options:
United Healthcare
Effective 8-1-25 H.S.A Plan HMO Value Premier
Bi-Weekly (26) Per Pay Period Plan A Plan B Plan
We offer our full-time employees and
Employee Only $ 68.23 $ 98.21 $116.05 $146.16 their eligible dependents coverage.
Children can join or remain on a
Employee + Spouse $275.32 $371.72 $409.26 $468.63
parent’s medical plan until age 26.
Employee + Child(ren) $238.55 $295.50 $325.50 $373.16 When a child turns 26, they will lose
medical coverage on the last day of
Employee + Family $390.64 $463.19 $538.26 $626.32 their birth month.
H.S.A Plan Navigate HMO
Brief Member NavE5000i10021B Choice E5000i8021B Choice E3000i8021B
Choice HE635025B
In-Network $6,350 Deductible $5,000 Deductible $5,000 Deductible $3,000 Deductible
Summary IN-NETWORK ONLY IN-NETWORK ONLY IN-NETWORK ONLY IN-NETWORK ONLY
PREMIER option with NO Specialist
LOW COST—HMO option with FIRST MID-RANGE—FIRST Dollar coverage
Referral Required. FISRT Dollar cover-
Difference Between HSA-Compatible High Deductible Dollar coverage with Copays (CYD Waived) with Copays (CYD Waived) on MOST age with Copays (CYD Waived) on MOST
Health Plans (HDHP) Lower
Plans Costs and Annual Out of Pocket on MOST Day to Day Services. Referral Day to Day Services. NO Specialist Day to Day Services. Lower Calendar
Required for Specialist Referral Required.
Year Deductible
Network CHOICE Navigate “TEXAS—Only” CHOICE CHOICE
(CYD) Calendar Year Individual: $6,350 Individual: $5,000 Individual: $5,000 Individual: $3,000
Family: $12,700 Family: $10,000 Family: $10,000 Family: $6,000
Deductible (Jan .1st to Dec. 31st)
Coinsurance Carrier: 100% Carrier: 100% Carrier: 80% Carrier: 80%
(After CYD) Member: 0% Member: 0% Member: 20% Member: 20%
Annual (OOP) Out of Individual: $6,350 Individual: $8,150 Individual: $8,150 Individual: $8,150
Pocket Maximum Family: 12,700 Family: $16,300 Family: $16,300 Family: $16,300
(PCP) Primary Care Under Age 19: $0 Copay Under Age 19: $0 Copay Under Age 19: $0 Copay
0% after CYD
Physician Over Age 19: $25 Copay Over Age 19: $25 Copay Over Age 19: $25 Copay
Specialist Physicians 0% after CYD $75 Copay $75 Copay $75 Copay
and Providers
YES, Not needed for (OB/GYN’s).,
Referral Required for NO Urgent Care, Behavioral health or NO NO
Specialists use disorder clinicians.
Dr. Consultation Virtual Member Pays $54
Visits, See Pg. 8 Cost Per Consultation $0 Copay $0 Copay $0 Copay
Basic: Lab, X-Rays &
Diagnostic Tests 0% after CYD Paid 100% No Charge Paid 100% No Charge Paid 100% No Charge
Major: Diagnostic & Calendar Year Deductible 20% after Calendar Year 20% after Calendar Year
Imaging 0% after CYD Applies Deductible (CYD) Deductible (CYD
Annual Preventive Care Covered 100% Covered 100% Covered 100% Covered 100%
Certain Rx are covered too,
See Page 5 (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays) (No CYD, Co-Ins. Copays)
Urgent Care 0% after CYD $50 copay $50 copay $50 copay
Emergency Room 0% after CYD $300 Copay, after CYD $300 Copay, 20% after CYD $300 Copay, 20% after CYD
Hospitalization: 0% after CYD 0% after CYD 20% after CYD / 20% after CYD
In / Outpatient (you must have a referral from your PCP) $250 Copay Applies
Prescription Drugs - 31 Tier 1 $10 Copay r 1 $10 Copay r 1 $10 Copay
i
e
T
e
i
T
Day Supply Retail
i
T
0% after CYD Tier 2 $35Copay r 2 $35Copay r 2 $35Copay
e
e
T
i
90 Day Supply Mail Tier 3 $75 Copay Tier 3 $75 Copay Tier 3 $75 Copay
Order at 2.5 Times Tier 4 $250 Copay Tier 4 $250 Copay Tier 4 $250 Copay
Retail
Specialty Drugs Own Copays Specialty Drugs Own Copays Specialty Drugs Own Copays
4 NOTE: This is only a brief overview. Please see Benefit Summary and SBC for more details. Please Register and use UHC Member www.myuhc.com or
Customer Service Toll Free 866-633-2446, for Navigate 855-828-7715 , for H.S.A 866-314-0335