
Page 4 - Letterpress 2021 Benefit Guide
P. 4
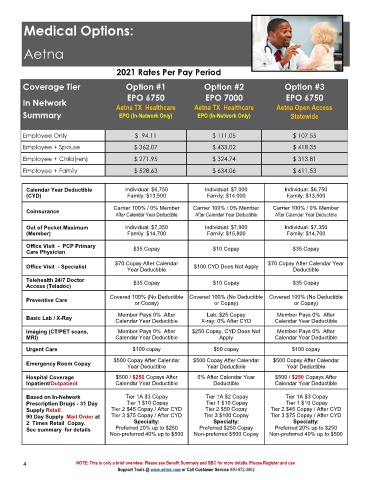
Medical Options:
Aetna
2021 Rates Per Pay Period
Coverage Tier Option #1 Option #2 Option #3
EPO 6750 EPO 7000 EPO 6750
In Network Aetna TX Healthcare Aetna TX Healthcare Aetna Open Access
Summary EPO (In-Network Only) EPO (In-Network Only) Statewide
Employee Only $ 94.11 $ 111.05 $ 107.55
Employee + Spouse $ 362.07 $ 433.02 $ 418.35
Employee + Child(ren) $ 271.95 $ 324.74 $ 313.81
Employee + Family $ 528.63 $ 634.06 $ 611.53
Calendar Year Deductible Individual: $6,750 Individual: $7,000 Individual: $6,750
(CYD) Family: $13,500 Family: $14,000 Family: $13,500
Carrier 100% / 0% Member Carrier 100% / 0% Member Carrier 100% / 0% Member
Coinsurance
After Calendar Year Deductible After Calendar Year Deductible After Calendar Year Deductible
Out of Pocket Maximum Individual: $7,350 Individual: $7,900 Individual: $7,350
(Member) Family: $14,700 Family: $15,800 Family: $14,700
Office Visit - PCP Primary $35 Copay $10 Copay $35 Copay
Care Physician
$70 Copay After Calendar $70 Copay After Calendar Year
Office Visit - Specialist $100 CYD Does Not Apply
Year Deductible Deductible
Telehealth 24/7 Doctor $35 Copay $10 Copay $35 Copay
Access (Teladoc)
Covered 100% (No Deductible Covered 100% (No Deductible Covered 100% (No Deductible
Preventive Care
or Copay) or Copay) or Copay)
Member Pays 0% After Lab: $25 Copay Member Pays 0% After
Basic Lab / X-Ray
Calendar Year Deductible X-ray: 0% After CYD Calendar Year Deductible
Imaging (CT/PET scans, Member Pays 0% After $250 Copay, CYD Does Not Member Pays 0% After
MRI) Calendar Year Deductible Apply Calendar Year Deductible
Urgent Care $100 copay $50 copay $100 copay
$500 Copay After Calendar $500 Copay After Calendar $500 Copay After Calendar
Emergency Room Copay
Year Deductible Year Deductible Year Deductible
5
$
Hospital Coverage $500 / $250 Copays After 0% After Calendar Year 00 / $250 Copays After
Inpatient/Outpatient Calendar Year Deductible Deductible Calendar Year Deductible
Based on In-Network Tier 1A $3 Copay Tier 1A $2 Copay Tier 1A $3 Copay
Prescription Drugs - 31 Day Tier 1 $10 Copay Tier 1 $10 Copay Tier 1 $10 Copay
i
r 2
e
T
y
p
Af
/
a
y
t
4
$
5
o
C
r 2
$
T
i
e
5
o
p
a
C
0
Supply Retail Tier 2 $45 Copay / After CYD er CYD
$
i
T
r 3
i
T
r 3
e
e
90 Day Supply Mail Order at Tier 3 $75 Copay / After CYD $100 Copay 75 Copay / After CYD
2 Times Retail Copay. Specialty: Specialty: Specialty:
See summary for details Preferred 20% up to $250 Preferred $250 Copay Preferred 20% up to $250
Non-preferred 40% up to $500 Non-preferred $500 Copay Non-preferred 40% up to $500
4 NOTE: This is only a brief overview. Please see Benefit Summary and SBC for more details. Please Register and use
Support Tools @ www.aetna.com or Call Customer Service 800-872-3862