
Page 31 - Planning Your Legacy VA Survivors and Burial Benefits Kit - January 2018
P. 31
OMB Number 2900-0219
Estimated Burden: 10 minutes
Expiration Date: 01/31/2017
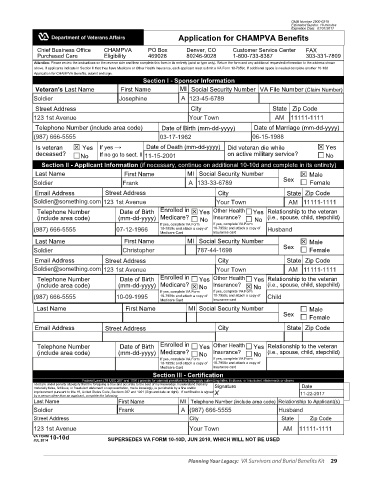
Application for CHAMPVA Benefits
Chief Business Office CHAMPVA PO Box Denver, CO Customer Service Center FAX
Purchased Care Eligibility 469028 80246-9028 1-800-733-8387 303-331-7809
Attention: Please review the instructions on the reverse side and then complete this form in its entirety (print or type only). Return the form and any additional requested information to the address shown
above. If applicants indicate in Section II that they have Medicare or Other Health Insurance, each applicant must submit a VA Form 10-7959c. If additional space is needed complete another 10-10d
Application for CHAMPVA Benefits, submit and sign.
Section I - Sponsor Information
Veteran's Last Name First Name MI Social Security Number VA File Number (Claim Number)
Soldier Josephine A 123-45-6789
Street Address City State Zip Code
123 1st Avenue Your Town AM 11111-1111
Telephone Number (include area code) Date of Birth (mm-dd-yyyy) Date of Marriage (mm-dd-yyyy)
SAMPLE
(987) 666-5555 03-17-1962 06-15-1988
Is veteran Yes If yes → Date of Death (mm-dd-yyyy) Did veteran die while Yes
deceased? No If no go to sect. II 11-15-2001 on active military service? No
Section II - Applicant Information (if necessary, continue on additional 10-10d and complete in its entirety)
Last Name First Name MI Social Security Number Male
Soldier Frank A 133-33-6789 Sex Female
Email Address Street Address City State Zip Code
Soldier@something.com 123 1st Avenue Your Town AM 11111-1111
Telephone Number Date of Birth Enrolled in Yes Other Health Yes Relationship to the veteran
(include area code) (mm-dd-yyyy) Medicare? No Insurance? No (i.e., spouse, child, stepchild)
If yes, complete VA Form If yes, complete VA Form
(987) 666-5555 07-12-1966 10-7959c and attach a copy of 10-7959c and attach a copy of Husband
Medicare Card Insurance card
Last Name First Name MI Social Security Number Male
Soldier Christopher 787-44-1698 Sex Female
Email Address Street Address City State Zip Code
Soldier@something.com 123 1st Avenue Your Town AM 11111-1111
Telephone Number Date of Birth Enrolled in Yes Other Health Yes Relationship to the veteran
(include area code) (mm-dd-yyyy) Medicare? No Insurance? No (i.e., spouse, child, stepchild)
If yes, complete VA Form If yes, complete VA Form
(987) 666-5555 10-09-1995 10-7959c and attach a copy of 10-7959c and attach a copy of Child
Medicare Card Insurance card
Last Name First Name MI Social Security Number Male
Sex Female
Email Address Street Address City State Zip Code
Telephone Number Date of Birth Enrolled in Yes Other Health Yes Relationship to the veteran
(include area code) (mm-dd-yyyy) Medicare? No Insurance? No (i.e., spouse, child, stepchild)
If yes, complete VA Form If yes, complete VA Form
10-7959c and attach a copy of 10-7959c and attach a copy of
Medicare Card Insurance card
Section III - Certification
Federal Laws (18 USC 287 and 1001) provide for criminal penalties for knowingly submitting false, fictitious, or fraudulent statements or claims
I declare under penalty of perjury that the foregoing is true and accurate to the best of my knowledge. I understand that any Signature Date
materially false, fictitious, or fraudulent statement or representation, made knowingly, is punishable by a fine and/or
imprisonment pursuant to title 18, United States Code, Sections 287 and 1001 (Sign and date on right). If certification is signed X 11-22-2017
by a person other than an applicant, complete the following:
Last Name First Name MI Telephone Number (include area code) Relationship to Applicant(s)
Soldier Frank A (987) 666-5555 Husband
Street Address City State Zip Code
123 1st Avenue Your Town AM 11111-1111
VA FORM 10-10d
JUL 2014 SUPERSEDES VA FORM 10-10D, JUN 2010, WHICH WILL NOT BE USED
Planning Your Legacy: VA Survivors and Burial Benefits Kit 29