
Page 5 - Flyer Employee Benefits Brochure FINAL 2021 CA w_compliance notices update 3_10
P. 5
Flyer Defense
2021–22 Employee Benefits Brochure
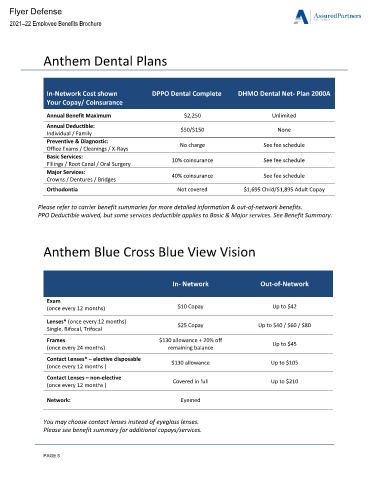
Anthem Dental Plans
In-Network Cost shown DPPO Dental Complete DHMO Dental Net- Plan 2000A
Your Copay/ Coinsurance
Annual Benefit Maximum $2,250 Unlimited
Annual Deductible: $50/$150 None
Individual / Family
Preventive & Diagnostic: No charge See fee schedule
Office Exams / Cleanings / X-Rays
Basic Services:
Fillings / Root Canal / Oral Surgery 10% coinsurance See fee schedule
Major Services: 40% coinsurance See fee schedule
Crowns / Dentures / Bridges
Orthodontia Not covered $1,695 Child/$1,895 Adult Copay
Please refer to carrier benefit summaries for more detailed information & out-of-network benefits.
PPO Deductible waived, but some services deductible applies to Basic & Major services. See Benefit Summary.
Anthem Blue Cross Blue View Vision
In- Network Out-of-Network
Exam
(once every 12 months) $10 Copay Up to $42
Lenses* (once every 12 months) $25 Copay Up to $40 / $60 / $80
Single, Bifocal, Trifocal
Frames $130 allowance + 20% off
(once every 24 months) remaining balance Up to $45
Contact Lenses* – elective disposable
(once every 12 months ) $130 allowance Up to $105
Contact Lenses – non-elective Covered in full Up to $210
(once every 12 months )
Network: Eyemed
You may choose contact lenses instead of eyeglass lenses.
Please see benefit summary for additional copays/services.
PAGE 5