
Page 6 - VSolvit 2021 EB Brochure_Updated Aug 2021
P. 6
VSolvit
2021 Employee Benefits Brochure
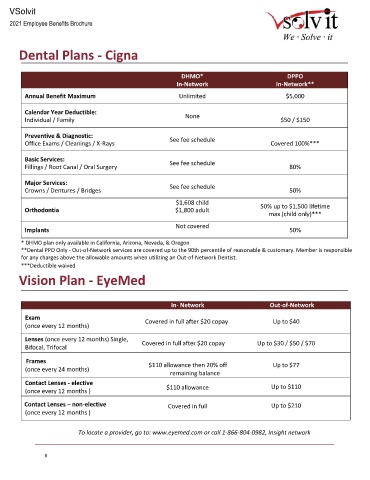
Dental Plans - Cigna
DHMO* DPPO
In-Network In-Network**
Annual Benefit Maximum Unlimited $5,000
Calendar Year Deductible:
Individual / Family None $50 / $150
Preventive & Diagnostic:
Office Exams / Cleanings / X-Rays See fee schedule Covered 100%***
Basic Services: See fee schedule
Fillings / Root Canal / Oral Surgery 80%
Major Services: See fee schedule
Crowns / Dentures / Bridges 50%
$1,608 child
Orthodontia $1,800 adult 50% up to $1,500 lifetime
max (child only)***
Not covered
Implants 50%
* DHMO plan only available in California, Arizona, Nevada, & Oregon
**Dental PPO Only - Out-of-Network services are covered up to the 90th percentile of reasonable & customary. Member is responsible
for any charges above the allowable amounts when utilizing an Out-of-Network Dentist.
***Deductible waived
Vision Plan - EyeMed
In- Network Out-of-Network
Exam Covered in full after $20 copay Up to $40
(once every 12 months)
Lenses (once every 12 months) Single,
Bifocal, Trifocal Covered in full after $20 copay Up to $30 / $50 / $70
Frames
$110 allowance then 20% off Up to $77
(once every 24 months)
remaining balance
Contact Lenses - elective Up to $110
(once every 12 months ) $110 allowance
Contact Lenses – non-elective Covered in full Up to $210
(once every 12 months )
To locate a provider, go to: www.eyemed.com or call 1-866-804-0982, Insight network
6