
Page 7 - 2021 HN Benefits Booklet
P. 7
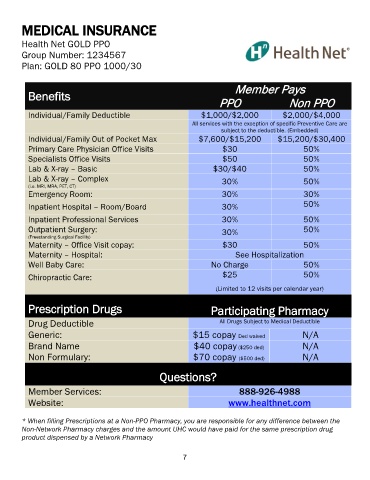
MEDICAL INSURANCE
Health Net GOLD PPO
Group Number: 1234567
Plan: GOLD 80 PPO 1000/30
Member Pays
Benefits
PPO Non PPO
Individual/Family Deductible $1,000/$2,000 $2,000/$4,000
All services with the exception of specific Preventive Care are
subject to the deductible. (Embedded)
Individual/Family Out of Pocket Max $7,600/$15,200 $15,200/$30,400
Primary Care Physician Office Visits $30 50%
Specialists Office Visits $50 50%
Lab & X-ray – Basic $30/$40 50%
Lab & X-ray – Complex 30%
(i.e. MRI, MRA, PET, CT) 50%
Emergency Room: 30% 30%
Inpatient Hospital – Room/Board 30% 50%
Inpatient Professional Services 30% 50%
Outpatient Surgery: 30% 50%
(Freestanding Surgical Facility)
Maternity – Office Visit copay: $30 50%
Maternity – Hospital: See Hospitalization
Well Baby Care: No Charge 50%
Chiropractic Care: $25 50%
(Limited to 12 visits per calendar year)
Prescription Drugs Participating Pharmacy
Drug Deductible All Drugs Subject to Medical Deductible
Generic: $15 copay Ded waived N/A
Brand Name $40 copay ($250 ded) N/A
Non Formulary: $70 copay ($500 ded) N/A
Questions?
Member Services: 888-926-4988
Website: www.healthnet.com
* When filling Prescriptions at a Non-PPO Pharmacy, you are responsible for any difference between the
Non-Network Pharmacy charges and the amount UHC would have paid for the same prescription drug
product dispensed by a Network Pharmacy
7