
Page 17 - CASA Bulletin of Anesthesiology 2022; 9(2) (5)
P. 17
Vol. 9, No 2, 2022
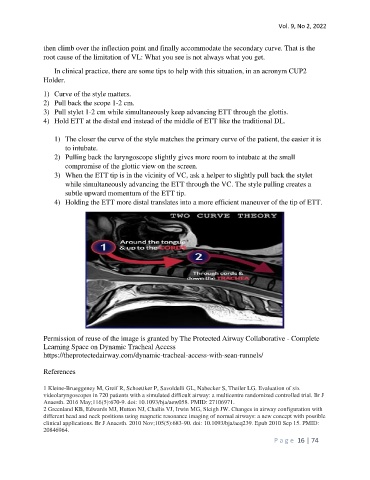
then climb over the inflection point and finally accommodate the secondary curve. That is the
root cause of the limitation of VL: What you see is not always what you get.
In clinical practice, there are some tips to help with this situation, in an acronym CUP2
Holder.
1) Curve of the style matters.
2) Pull back the scope 1-2 cm.
3) Pull stylet 1-2 cm while simultaneously keep advancing ETT through the glottis.
4) Hold ETT at the distal end instead of the middle of ETT like the traditional DL.
1) The closer the curve of the style matches the primary curve of the patient, the easier it is
to intubate.
2) Pulling back the laryngoscope slightly gives more room to intubate at the small
compromise of the glottic view on the screen.
3) When the ETT tip is in the vicinity of VC, ask a helper to slightly pull back the stylet
while simultaneously advancing the ETT through the VC. The style pulling creates a
subtle upward momentum of the ETT tip.
4) Holding the ETT more distal translates into a more efficient maneuver of the tip of ETT.
Permission of reuse of the image is granted by The Protected Airway Collaborative - Complete
Learning Space on Dynamic Tracheal Access
https://theprotectedairway.com/dynamic-tracheal-access-with-sean-runnels/
References
1 Kleine-Brueggeney M, Greif R, Schoettker P, Savoldelli GL, Nabecker S, Theiler LG. Evaluation of six
videolaryngoscopes in 720 patients with a simulated difficult airway: a multicentre randomized controlled trial. Br J
Anaesth. 2016 May;116(5):670-9. doi: 10.1093/bja/aew058. PMID: 27106971.
2 Greenland KB, Edwards MJ, Hutton NJ, Challis VJ, Irwin MG, Sleigh JW. Changes in airway configuration with
different head and neck positions using magnetic resonance imaging of normal airways: a new concept with possible
clinical applications. Br J Anaesth. 2010 Nov;105(5):683-90. doi: 10.1093/bja/aeq239. Epub 2010 Sep 15. PMID:
20846964.
P a g e 16 | 74