
Page 5 - Interwest Benefits Guide
P. 5
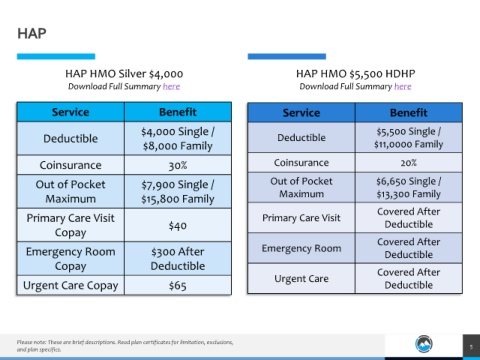
HAP
HAP HMO Silver $4,000 HAP HMO $5,500 HDHP
Download Full Summary here Download Full Summary here
Service Benefit Service Benefit
$4,000 Single / $5,500 Single /
Deductible Deductible
$8,000 Family $11,0000 Family
Coinsurance 30% Coinsurance 20%
Out of Pocket $7,900 Single / Out of Pocket $6,650 Single /
Maximum $13,300 Family
Maximum $15,800 Family
Covered After
Primary Care Visit Primary Care Visit
$40 Deductible
Copay
Covered After
Emergency Room $300 After Emergency Room Deductible
Copay Deductible Covered After
Urgent Care
Urgent Care Copay $65 Deductible
Please note: These are brief descriptions. Read plan certificates for limitation, exclusions,
5
and plan specifics.