
Page 3 - Sparky's Electric - 2020 Renewal Presentation
P. 3
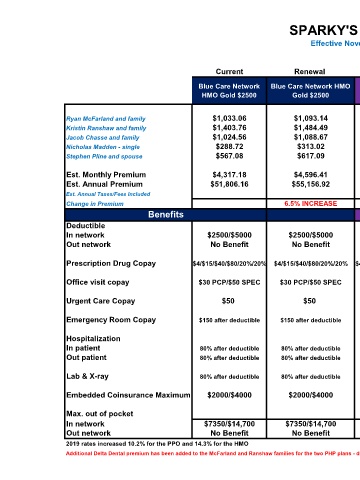
SPARKY'S ELECTRIC
Effective November 1, 2020
Current Renewal Alt # 1 Alt # 2 Alt # 3 Alt # 4
Blue Care Network
Blue Care Network Blue Care Network HMO HMO PCP Focus Blue Care Network PHP HMO Gold $2000 PHP HMO Silver
HMO Gold $2500 Gold $2500 Gold $2500 HMO Gold $3000 $3000
Ryan McFarland and family $1,033.06 $1,093.14 $1,007.96 $1,057.88 $1,092.59 $917.73
Kristin Ranshaw and family $1,403.76 $1,484.49 $1,367.93 $1,436.25 $1,476.49 $1,237.24
Jacob Chasse and family $1,024.56 $1,088.67 $1,003.84 $1,053.48 $1,038.35 $864.23
Nicholas Madden - single $288.72 $313.02 $287.93 $302.63 $307.06 $255.57
Stephen Pline and spouse $567.08 $617.09 $567.63 $596.61 $605.34 $503.83
Est. Monthly Premium $4,317.18 $4,596.41 $4,235.29 $4,446.85 $4,519.83 $3,778.60
Est. Annual Premium $51,806.16 $55,156.92 $50,823.48 $53,362.20 $54,237.96 $45,343.20
Est. Annual Taxes/Fees Included
Change in Premium 6.5% INCREASE SAVE 1.9% 3% INCREASE 4.7% INCREASE SAVE 12.5%
Benefits
Deductible
In network $2500/$5000 $2500/$5000 $2500/$5000 $3000/$6000 $2000/$4000 $3000/$6000
Out network No Benefit No Benefit No Benefit No Benefit No Benefit No Benefit
Prescription Drug Copay $4/$15/$40/$80/20%/20% $4/$15/$40/$80/20%/20% $4/$15/$40/$80/20%/20%$4/$15/$40/$80/20%/20% $20/$50/$80/20%/20% $40/$80/$200/20%/20%
Office visit copay $30 PCP/$50 SPEC $30 PCP/$50 SPEC $30 PCP/$50 SPEC $30 PCP/$50 SPEC $25 PCP/$50 SPEC $45 PCP/$65 SPEC
Urgent Care Copay $50 $50 $50 $50 $60 $65
Emergency Room Copay $150 after deductible $150 after deductible $150 after deductible $150 after deductible 20% after deductible 70% after deductible
Hospitalization
In patient 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 70% after deductible
Out patient 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 70% after deductible
Lab & X-ray 80% after deductible 80% after deductible 80% after deductible 80% after deductible 80% after deductible 70% after deductible
Embedded Coinsurance Maximum $2000/$4000 $2000/$4000 $2000/$4000 $3000/$6000 $1500/$3000 N/A
Max. out of pocket
In network $7350/$14,700 $7350/$14,700 $7350/$14,700 $8150/$16,300 $8000/$16,000 $8000/$16,000
Out network No Benefit No Benefit No Benefit No Benefit No Benefit No Benefit
2019 rates increased 10.2% for the PPO and 14.3% for the HMO Prepared August 2020
Additional Delta Dental premium has been added to the McFarland and Ranshaw families for the two PHP plans - due to pediatric dental