
Page 5 - Affiliate Mortgage Services September 2020 Renewal
P. 5
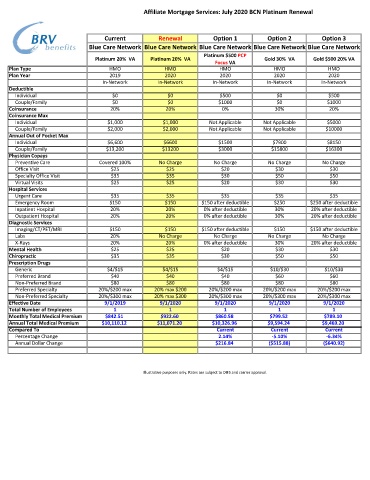
Affiliate Mortgage Services: July 2020 BCN Platinum Renewal
Current Renewal Option 1 Option 2 Option 3
Blue Care Network Blue Care Network Blue Care Network Blue Care Network Blue Care Network
Platinum $500 PCP
Platinum 20% VA Platinum 20% VA Gold 30% VA Gold $500 20% VA
Focus VA
Plan Type HMO HMO HMO HMO HMO
Plan Year 2019 2020 2020 2020 2020
In-Network In-Network In-Network In-Network In-Network
Deductible
Individual $0 $0 $500 $0 $500
Couple/Family $0 $0 $1000 $0 $1000
Coinsurance 20% 20% 0% 30% 20%
Coinsurance Max
Individual $1,000 $1,000 Not Applicable Not Applicable $5000
Couple/Family $2,000 $2,000 Not Applicable Not Applicable $10000
Annual Out of Pocket Max
Individual $6,600 $6600 $1500 $7900 $8150
Couple/Family $13,200 $13200 $3000 $15800 $16300
Physician Copays
Preventive Care Covered 100% No Charge No Charge No Charge No Charge
Office Visit $25 $25 $20 $30 $30
Specialty Office Visit $35 $35 $30 $50 $50
Virtual Visits $25 $25 $20 $30 $30
Hospital Services
Urgent Care $35 $35 $35 $35 $35
Emergency Room $150 $150 $150 after deductible $250 $250 after deductible
Inpatient Hospital 20% 20% 0% after deductible 30% 20% after deductible
Outpatient Hospital 20% 20% 0% after deductible 30% 20% after deductible
Diagnostic Services
Imaging/CT/PET/MRI $150 $150 $150 after deductible $150 $150 after deductible
Labs 20% No Charge No Charge No Charge No Charge
X-Rays 20% 20% 0% after deductible 30% 20% after deductible
Mental Health $25 $25 $20 $30 $30
Chiropractic $35 $35 $30 $50 $50
Prescription Drugs
Generic $4/$15 $4/$15 $4/$15 $10/$30 $10/$30
Preferred Brand $40 $40 $40 $60 $60
Non-Preferred Brand $80 $80 $80 $80 $80
Preferred Specialty 20%/$200 max 20% max $200 20%/$200 max 20%/$200 max 20%/$200 max
Non-Preferred Specialty 20%/$300 max 20% max $300 20%/$300 max 20%/$300 max 20%/$300 max
Effective Date 9/1/2019 9/1/2020 9/1/2020 9/1/2020 9/1/2020
Total Number of Employees 1 1 1 1 1
Monthly Total Medical Premium $842.51 $922.60 $860.58 $799.52 $789.10
Annual Total Medical Premium $10,110.12 $11,071.20 $10,326.96 $9,594.24 $9,469.20
Compared To Current Current Current
Percentage Change 2.14% -5.10% -6.34%
Annual Dollar Change $216.84 ($515.88) ($640.92)
Illustrative purposes only. Rates are subject to DIFS and carrier approval.