
Page 3 - GMEI Benefits Guide 2020
P. 3
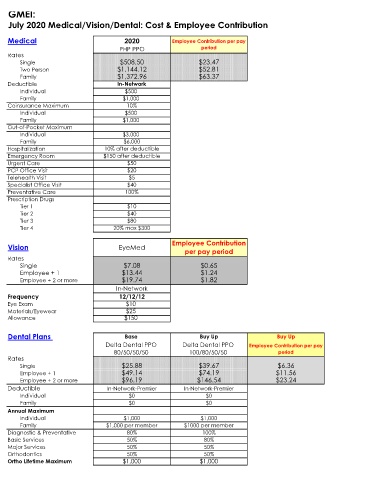
GMEI:
July 2020 Medical/Vision/Dental: Cost & Employee Contribution
Medical 2020 Employee Contribution per pay
PHP PPO period
Rates
Single $508.50 $23.47
Two Person $1,144.12 $52.81
Family $1,372.96 $63.37
Deductible In-Network
Individual $500
Family $1,000
Coinsurance Maximum 10%
Individual $500
Family $1,000
Out-of-Pocket Maximum
Individual $3,000
Family $6,000
Hospitalization 10% after deductible
Emergency Room $150 after deductible
Urgent Care $50
PCP Office Visit $20
Telehealth Visit $5
Specialist Office Visit $40
Preventative Care 100%
Prescription Drugs
Tier 1 $10
Tier 2 $40
Tier 3 $80
Tier 4 20% max $300
Vision EyeMed Employee Contribution
per pay period
Rates
Single $7.08 $0.65
Employee + 1 $13.44 $1.24
Employee + 2 or more $19.74 $1.82
In-Network
Frequency 12/12/12
Eye Exam $10
Materials/Eyewear $25
Allowance $150
Dental Plans Base Buy Up Buy Up
Delta Dental PPO Delta Dental PPO Employee Contribution per pay
80/50/50/50 100/80/50/50 period
Rates
Single $25.88 $39.67 $6.36
Employee + 1 $49.14 $74.19 $11.56
Employee + 2 or more $96.19 $146.54 $23.24
Deductible In-Network-Premier In-Network-Premier
Individual $0 $0
Family $0 $0
Annual Maximum
Individual $1,000 $1,000
Family $1,000 per member $1000 per member
Diagnostic & Preventative 80% 100%
Basic Services 50% 80%
Major Services 50% 50%
Orthodontics 50% 50%
Ortho Lifetime Maximum $1,000 $1,000