
Page 20 - QCS.19 SPD - HSA
P. 20
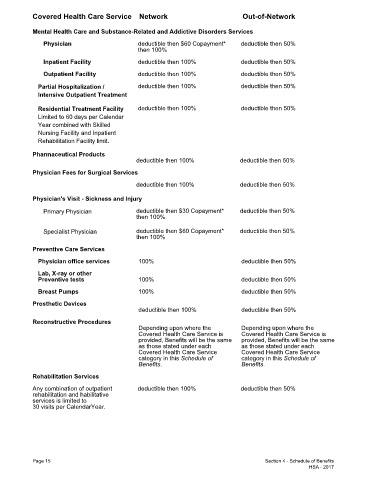
Covered Health Care Service Network Out-of-Network
Mental Health Care and Substance-Related and Addictive Disorders Services
Physician deductible then $60 Copayment* deductible then 50%
then 100%
Inpatient Facility deductible then 100% deductible then 50%
Outpatient Facility deductible then 100% deductible then 50%
Partial Hospitalization / deductible then 100% deductible then 50%
Intensive Outpatient Treatment
Residential Treatment Facility deductible then 100% deductible then 50%
Limited to 60 days per Calendar
Year combined with Skilled
Nursing Facility and Inpatient
Rehabilitation Facility limit.
Pharmaceutical Products
deductible then 100% deductible then 50%
Physician Fees for Surgical Services
deductible then 100% deductible then 50%
Physician's Visit - Sickness and Injury
Primary Physician deductible then $30 Copayment* deductible then 50%
then 100%
Specialist Physician deductible then $60 Copayment* deductible then 50%
then 100%
Preventive Care Services
Physician office services 100% deductible then 50%
Lab, X-ray or other
Preventive tests 100% deductible then 50%
Breast Pumps 100% deductible then 50%
Prosthetic Devices
deductible then 100% deductible then 50%
Reconstructive Procedures
Depending upon where the Depending upon where the
Covered Health Care Service is Covered Health Care Service is
provided, Benefits will be the same provided, Benefits will be the same
as those stated under each as those stated under each
Covered Health Care Service Covered Health Care Service
category in this Schedule of category in this Schedule of
Benefits. Benefits.
Rehabilitation Services
Any combination of outpatient deductible then 100% deductible then 50%
rehabilitation and habilitative
services is limited to
30 visits per CalendarYear.
Page 15 Section 4 - Schedule of Benefits
HSA - 2017