
Page 29 - PWH.19 Employee Benefits
P. 29
2019 Dental Benefits
Dental Care Plus
HMO Dental Plan
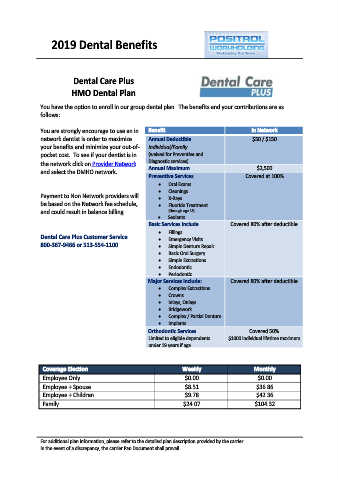
You have the option to enroll in our group dental plan. The benefits and your contributions are as
follows:
You are strongly encourage to use an in Benefit In Network
network dentist is order to maximize Annual Deductible $50 / $150
your benefits and minimize your out-of- Individual/Family
pocket cost. To see if your dentist is in (waived for Preventive and
the network click on Provider Network Diagnostic services)
and select the DMHO network. Annual Maximum $2,500
Preventive Services Covered at 100%
Oral Exams
•
• Cleanings
Payment to Non Network providers will • X-Rays
be based on the Network fee schedule, • Fluoride Treatment
and could result in balance billing. • (through age 18)
Sealants
Basic Services Include Covered 80% after deductible
• Fillings
Dental Care Plus Customer Service • Emergency Visits
800-367-9466 or 513-554-1100 • Simple Denture Repair
• Basic Oral Surgery
• Simple Extractions
• Endodontic
• Periodontic
Major Services Include: Covered 80% after deductible
• Complex Extractions
• Crowns
• Inlays, Onlays
• Bridgework
• Complex / Partial Denture
• Implants
Orthodontic Services Covered 50%
Limited to eligible dependents $1000 individual lifetime maximum
under 19 years if age
Coverage Election Weekly Monthly
Employee Only $0.00 $0.00
Employee + Spouse $8.51 $36.86
Employee + Children $9.78 $42.36
Family $24.07 $104.32
For additional plan information, please refer to the detailed plan description provided by the carrier.
In the event of a discrepancy, the carrier Pan Document shall prevail.