
Page 7 - LRM.19 Principal Employee Packet
P. 7
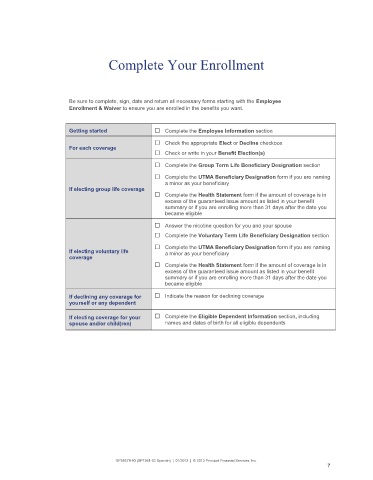
Complete Your Enrollment
Be sure to complete, sign, date and return all necessary forms starting with the Employee
Enrollment & Waiver to ensure you are enrolled in the benefits you want.
Getting started □ Complete the Employee Information section
□ Check the appropriate Elect or Decline checkbox
For each coverage
□ Check or write in your Benefit Election(s)
□ Complete the Group Term Life Beneficiary Designation section
□ Complete the UTMA Beneficiary Designation form if you are naming
a minor as your beneficiary
If electing group life coverage
□ Complete the Health Statement form if the amount of coverage is in
excess of the guaranteed issue amount as listed in your benefit
summary or if you are enrolling more than 31 days after the date you
became eligible
□ Answer the nicotine question for you and your spouse
□ Complete the Voluntary Term Life Beneficiary Designation section
□ Complete the UTMA Beneficiary Designation form if you are naming
If electing voluntary life a minor as your beneficiary
coverage
□ Complete the Health Statement form if the amount of coverage is in
excess of the guaranteed issue amount as listed in your benefit
summary or if you are enrolling more than 31 days after the date you
became eligible
If declining any coverage for □ Indicate the reason for declining coverage
yourself or any dependent
If electing coverage for your □ Complete the Eligible Dependent Information section, including
spouse and/or child(ren) names and dates of birth for all eligible dependents
GP59579-03 (SP1361-02 Spanish) | 01/2013 | © 2013 Principal Financial Services, Inc.
7