
Page 21 - Demo
P. 21
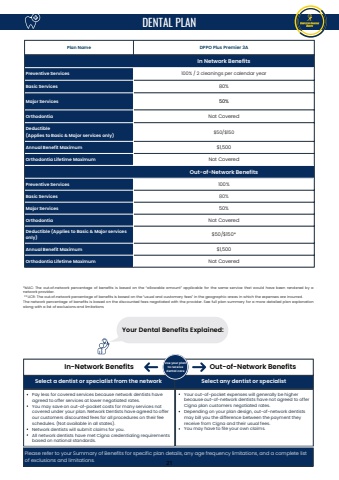
Plan Name DPPO Plus Premier 3AIn Network BenefitsPreventive Services 100% / 2 cleanings per calendar yearBasic Services 80%Major Services 50%Orthodontia Not CoveredDeductible(Applies to Basic & Major services only) $50/$150Annual Benefit Maximum $1,500Orthodontia Lifetime Maximum Not CoveredOut-of-Network BenefitsPreventive Services 100%Basic Services 80%Major Services 50%Orthodontia Not CoveredDeductible (Applies to Basic & Major servicesonly) $50/$150*Annual Benefit Maximum $1,500Orthodontia Lifetime Maximum Not Covered*MAC: The out%u2010of%u2010network percentage of benefits is based on the %u201callowable amount%u201d applicable for the same service that would have been rendered by anetwork provider.**UCR: The out%u2010of%u2010network percentage of benefits is based on the %u201cusual and customary fees%u201d in the geographic areas in which the expenses are incurred.The network percentage of benefits is based on the discounted fees negotiated with the provider. See full plan summary for a more detailed plan explanationalong with a list of exclusions and limitationsDENTAL PLANIn-Network Benefits Out-of-Network BenefitsSelect a dentist or specialist from the network Select any dentist or specialistPay less for covered services because network dentists haveagreed to offer services at lower negotiated rates.You may save on out-of-pocket costs for many services notcovered under your plan. Network Dentists have agreed to offerour customers discounted fees for all procedures on their feeschedules. (Not available in all states).Network dentists will submit claims for you.All network dentists have met Cigna credentialing requirementsbased on national standards.Your out-of-pocket expenses will generally be higherbecause out-of-network dentists have not agreed to offerCigna plan customers negotiated rates.Depending on your plan design, out-of-network dentistsmay bill you the difference between the payment theyreceive from Cigna and their usual fees.You may have to file your own claims.Please refer to your Summary of Benefits for specific plan details, any age frequency limitations, and a complete listof exclusions and limitations.Use your planto receivedental careYour Dental Benefits Explained:21
