
Page 31 - Demo
P. 31
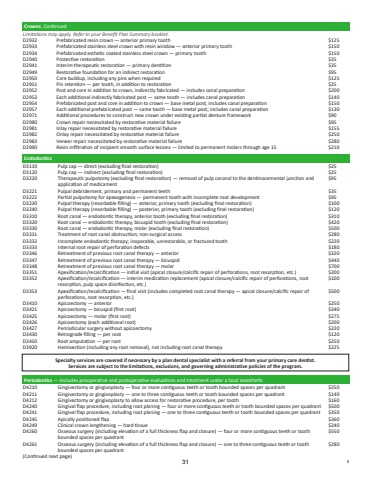
EndodonticsD3110 Pulp cap %u2014 direct (excluding final restoration) $25D3120 Pulp cap %u2014 indirect (excluding final restoration) $25D3220 Therapeutic pulpotomy (excluding final restoration) %u2014 removal of pulp coronal to the dentinocemental junction and application of medicament$95D3221 Pulpal debridement, primary and permanent teeth $35D3222 Partial pulpotomy for apexogenesis %u2014 permanent tooth with incomplete root development $95D3230 Pulpal therapy (resorbable filling) %u2014 anterior, primary tooth (excluding final restoration) $100D3240 Pulpal therapy (resorbable filling) %u2014 posterior, primary tooth (excluding final restoration) $120D3310 Root canal %u2014 endodontic therapy, anterior tooth (excluding final restoration) $310D3320 Root canal %u2014 endodontic therapy, bicuspid tooth (excluding final restoration) $420D3330 Root canal %u2014 endodontic therapy, molar (excluding final restoration) $500D3331 Treatment of root canal obstruction; non-surgical access $280D3332 Incomplete endodontic therapy; inoperable, unrestorable, or fractured tooth $220D3333 Internal root repair of perforation defects $180D3346 Retreatment of previous root canal therapy %u2014 anterior $320D3347 Retreatment of previous root canal therapy %u2014 bicuspid $440D3348 Retreatment of previous root canal therapy %u2014 molar $700D3351 Apexification/recalcification %u2014 initial visit (apical closure/calcific repair of perforations, root resorption, etc.) $200D3352 Apexification/recalcification %u2014 interim medication replacement (apical closure/calcific repair of perforations, root resorption, pulp space disinfection, etc.)$100D3353 Apexification/recalcification %u2014 final visit (includes completed root canal therapy %u2014 apical closure/calcific repair of perforations, root resorption, etc.)$500D3410 Apicoectomy %u2014 anterior $250D3421 Apicoectomy %u2014 bicuspid (first root) $340D3425 Apicoectomy %u2014 molar (first root) $275D3426 Apicoectomy (each additional root) $200D3427 Periradicular surgery without apicoectomy $220D3430 Retrograde filling %u2014 per root $120D3450 Root amputation %u2014 per root $250D3920 Hemisection (including any root removal), not including root canal therapy $225Crowns, ContinuedLimitations may apply. Refer to your Benefit Plan Summary booklet.D2932 Prefabricated resin crown %u2014 anterior primary tooth $125D2933 Prefabricated stainless steel crown with resin window %u2014 anterior primary tooth $150D2934 Prefabricated esthetic coated stainless steel crown %u2014 primary tooth $150D2940 Protective restoration $35D2941 Interim therapeutic restoration %u2014 primary dentition $35D2949 Restorative foundation for an indirect restoration $95D2950 Core buildup, including any pins when required $125D2951 Pin retention %u2014 per tooth, in addition to restoration $25D2952 Post and core in addition to crown, indirectly fabricated %u2014 includes canal preparation $200D2953 Each additional indirectly fabricated post %u2014 same tooth %u2014 includes canal preparation $140D2954 Prefabricated post and core in addition to crown %u2014 base metal post; includes canal preparation $150D2957 Each additional prefabricated post %u2014 same tooth %u2014 base metal post; includes canal preparation $130D2971 Additional procedures to construct new crown under existing partial denture framework $90D2980 Crown repair necessitated by restorative material failure $95D2981 Inlay repair necessitated by restorative material failure $155D2982 Onlay repair necessitated by restorative material failure $250D2983 Veneer repair necessitated by restorative material failure $280D2990 Resin infiltration of incipient smooth surface lesions %u2014 limited to permanent molars through age 15 $210Periodontics %u2014 Includes preoperative and postoperative evaluations and treatment under a local anestheticD4210 Gingivectomy or gingivoplasty %u2014 four or more contiguous teeth or tooth bounded spaces per quadrant $250D4211 Gingivectomy or gingivoplasty %u2014 one to three contiguous teeth or tooth bounded spaces per quadrant $140D4212 Gingivectomy or gingivoplasty to allow access for restorative procedure, per tooth $160D4240 Gingival flap procedure, including root planing %u2014 four or more contiguous teeth or tooth bounded spaces per quadrant $500D4241 Gingival flap procedure, including root planing %u2014 one to three contiguous teeth or tooth bounded spaces per quadrant $350D4245 Apically positioned flap $360D4249 Clinical crown lengthening %u2014 hard tissue $240D4260 Osseous surgery (including elevation of a full thickness flap and closure) %u2014 four or more contiguous teeth or tooth bounded spaces per quadrant$550D4261 Osseous surgery (including elevation of a full thickness flap and closure) %u2014 one to three contiguous teeth or tooth bounded spaces per quadrant$280(Continued next page)Specialty services are covered if necessary by a plan dental specialist with a referral from your primary care dentist. Services are subject to the limitations, exclusions, and governing administrative policies of the program.313
