
Page 7 - Demo
P. 7
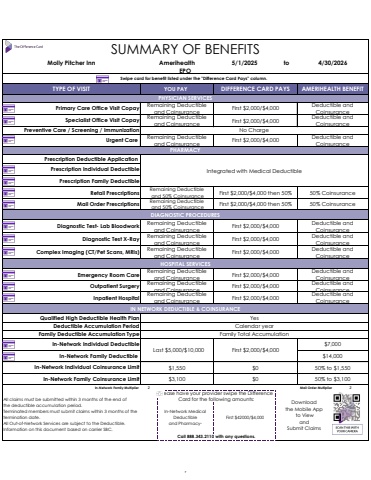
5/1/2025 toIn-Network Family Multiplier 2 Mail Order Multiplier 2Please have your provider swipe the Difference Card for the following amounts: Download the Mobile App to View and Submit ClaimsAll claims must be submitted within 3 months of the end of the deductible accumulation period.Terminated members must submit claims within 3 months of the termination date.All Out-of-Network Services are subject to the Deductible.Information on this document based on carrier SBC.Call 888.343.2110 with any questions.In-Network Medical Deductibleand PharmacyFirst $42000/$4,000In-Network Individual Coinsurance Limit $1,550 $0 50% to $1,550In-Network Family Coinsurance Limit $3,100 $0 50% to $3,100Family Deductible Accumulation Type In-Network Individual Deductible $7,000In-Network Family Deductible $14,000Family Total AccumulationLast $5,000/$10,000 First $2,000/$4,000Inpatient Hospital Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceIN NETWORK DEDUCTIBLE & COINSURANCEQualified High Deductible Health Plan YesDeductible Accumulation Period Calendar yearHOSPITAL SERVICESEmergency Room Care Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceOutpatient Surgery Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceDiagnostic Test- Lab Bloodwork Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceDiagnostic Test X-Ray Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceComplex Imaging (CT/Pet Scans, MRIs) Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceRetail Prescriptions Remaining Deductible and 50% Coinsurance First $2,000/$4,000 then 50% 50% CoinsuranceMail Order Prescriptions Remaining Deductible and 50% Coinsurance First $2,000/$4,000 then 50% 50% CoinsuranceDIAGNOSTIC PROCEDURESPHYSICIAN SERVICESPrimary Care Office Visit Copay Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsurancePHARMACYPrescription Deductible Application Prescription Individual DeductiblePrescription Family DeductibleIntegrated with Medical DeductibleSpecialist Office Visit Copay Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsurancePreventive Care / Screening / Immunization No ChargeUrgent Care Remaining Deductible and Coinsurance First $2,000/$4,000Deductible and CoinsuranceSUMMARY OF BENEFITSMolly Pitcher Inn Amerihealth 4/30/2026EPO Swipe card for benefit listed under the \TYPE OF VISIT YOU PAY DIFFERENCE CARD PAYS AMERIHEALTH BENEFIT7
