
Page 7 - Demo
P. 7
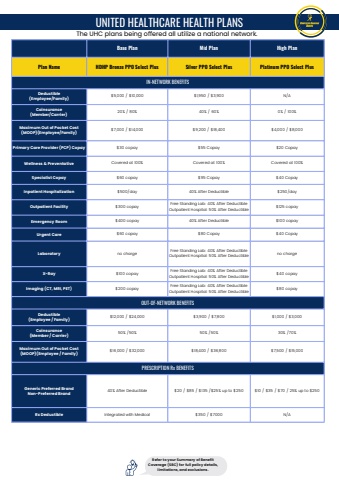
Base Plan Mid Plan High PlanPlan Name HDHP Bronze PPO Select Plus Silver PPO Select Plus Platinum PPO Select PlusIN-NETWORK BENEFITSDeductible(Employee/Family)$5,000 / $10,000 $1,950 / $3,900 N/ACoinsurance(Member/Carrier)20% / 80% 40% / 60% 0% / 100%Maximum Out of Pocket Cost(MOOP)(Employee/Family)$7,000 / $14,000 $9,200 / $18,400 $4,000 / $8,000Primary Care Provider (PCP) Copay $30 copay $55 Copay $20 CopayWellness & Preventative Covered at 100% Covered at 100% Covered at 100%Specialist Copay $60 copay $95 Copay $40 CopayInpatient Hospitalization $500/day 40% After Deductible $250/dayOutpatient Facility $300 copayFree Standing Lab: 40% After DeductibleOutpatient Hospital: 50% After Deductible$125 copayEmergency Room $400 copay 40% After Deductible $100 copayUrgent Care $60 copay $80 Copay $40 CopayLaboratory no chargeFree Standing Lab: 40% After DeductibleOutpatient Hospital: 50% After Deductibleno chargeX-Ray $100 copayFree Standing Lab: 40% After DeductibleOutpatient Hospital: 50% After Deductible$40 copayImaging (CT, MRI, PET) $200 copayFree Standing Lab: 40% After DeductibleOutpatient Hospital: 50% After Deductible$80 copayOUT-OF-NETWORK BENEFITSDeductible(Employee / Family)$12,000 / $24,000 $3,900 / $7,800 $1,000 / $3,000Coinsurance(Member / Carrier)50% /50% 50% /50% 30% /70%Maximum Out of Pocket Cost(MOOP)(Employee / Family)$16,000 / $32,000 $18,400 / $36,800 $7,500 / $15,000PRESCRIPTION Rx BENEFITSGeneric Preferred BrandNon-Preferred Brand40% After Deductible $20 / $85 / $135 /$25% up to $250 $10 / $35 / $70 / 25% up to $250Rx Deductible Integrated with Medical $350 / $7000 N/AUNITED HEALTHCARE HEALTH PLANSRefer to your Summary of BenefitCoverage (SBC) for full policy details,limitations, and exclusions.The UHC plans being offered all utilize a national network.
