
Page 44 - e-CPG-SLE-8_5_24
P. 44
Management of Systemic Lupus Erythematosus
8. SPECIFIC CLINICAL MANIFESTATIONS
SLE is a multisystemic disease requiring comprehensive treatment
which is determined by the disease severity and organ/system involved.
8.1 Lupus Nephritis
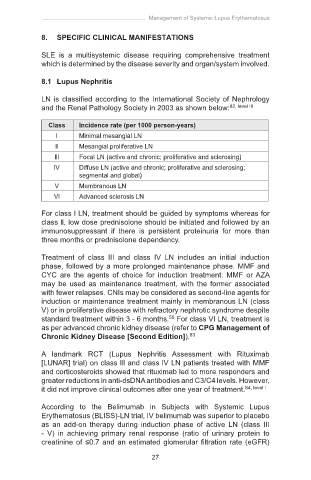
LN is classified according to the International Society of Nephrology
and the Renal Pathology Society in 2003 as shown below: 82, level III
Class Incidence rate (per 1000 person-years)
l Minimal mesangial LN
Il Mesangial proliferative LN
lll Focal LN (active and chronic; proliferative and sclerosing)
lV Diffuse LN (active and chronic; proliferative and sclerosing;
segmental and global)
V Membranous LN
Vl Advanced sclerosis LN
For class l LN, treatment should be guided by symptoms whereas for
class ll, low dose prednisolone should be initiated and followed by an
immunosuppressant if there is persistent proteinuria for more than
three months or prednisolone dependency.
Treatment of class III and class IV LN includes an initial induction
phase, followed by a more prolonged maintenance phase. MMF and
CYC are the agents of choice for induction treatment. MMF or AZA
may be used as maintenance treatment, with the former associated
with fewer relapses. CNIs may be considered as second-line agents for
induction or maintenance treatment mainly in membranous LN (class
V) or in proliferative disease with refractory nephrotic syndrome despite
standard treatment within 3 - 6 months. For class VI LN, treatment is
50
as per advanced chronic kidney disease (refer to CPG Management of
Chronic Kidney Disease [Second Edition]). 83
A landmark RCT (Lupus Nephritis Assessment with Rituximab
[LUNAR] trial) on class lll and class lV LN patients treated with MMF
and corticosteroids showed that rituximab led to more responders and
greater reductions in anti-dsDNA antibodies and C3/C4 levels. However,
it did not improve clinical outcomes after one year of treatment. 84, level l
According to the Belimumab in Subjects with Systemic Lupus
Erythematosus (BLISS)-LN trial, IV belimumab was superior to placebo
as an add-on therapy during induction phase of active LN (class III
- V) in achieving primary renal response (ratio of urinary protein to
creatinine of ≤0.7 and an estimated glomerular filtration rate (eGFR)
27