
Page 79 - Rapid Review of ECG Interpretation in Small Animal Practice, 2nd Edition
P. 79
Answers 18, 19 ECG Cases
Answer 18
VetBooks.ir 1 ECG 18 shows sinus rhythm with a left anterior fascicular block (LAFB) pattern.
2 • The heart rate is 200 bpm. The MEA is shifted to the left to –50° (see Section 2, Evaluation of the
Electrocardiogram). The QRS duration is 20 ms and normal.
• The LAFB pattern is thought to arise from disruption of the anterior fascicule of the left bundle branch
that supplies the cranial and basilar region of the left ventricle with electrical impulses. A region of
block will result in a deviation of the MEA of the ventricular depolarization to the left, but the QRS
duration is not prolonged since only one of the two fascicules of the left bundle branch is blocked.
• This conduction disturbance does not tend to progress to more advanced degrees of bundle branch
block and does not warrant any treatment per se; however, many cats with LAFB patterns are found
to have cardiomyopathy. This ECG finding in conjunction with the presence of a systolic murmur
warrants further diagnostics, such as thoracic radiography or echocardiography prior to general
anesthesia for a dental procedure.
Answer 19
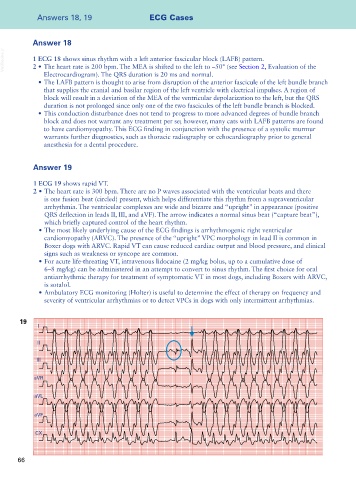
1 ECG 19 shows rapid VT.
2 • The heart rate is 300 bpm. There are no P waves associated with the ventricular beats and there
is one fusion beat (circled) present, which helps differentiate this rhythm from a supraventricular
arrhythmia. The ventricular complexes are wide and bizarre and “upright” in appearance (positive
QRS deflection in leads II, III, and aVF). The arrow indicates a normal sinus beat (“capture beat”),
which briefly captured control of the heart rhythm.
• The most likely underlying cause of the ECG findings is arrhythmogenic right ventricular
cardiomyopathy (ARVC). The presence of the “upright” VPC morphology in lead II is common in
Boxer dogs with ARVC. Rapid VT can cause reduced cardiac output and blood pressure, and clinical
signs such as weakness or syncope are common.
• For acute life-threating VT, intravenous lidocaine (2 mg/kg bolus, up to a cumulative dose of
6–8 mg/kg) can be administered in an attempt to convert to sinus rhythm. The first choice for oral
antiarrhythmic therapy for treatment of symptomatic VT in most dogs, including Boxers with ARVC,
is sotalol.
• Ambulatory ECG monitoring (Holter) is useful to determine the effect of therapy on frequency and
severity of ventricular arrhythmias or to detect VPCs in dogs with only intermittent arrhythmias.
19
I
II
III
aVR
aVL
aVF
CX
66