
Page 51 - Fluid, Electrolyte, and Acid-Base Disorders in Small Animal Practice
P. 51
40 APPLIED PHYSIOLOGY
and recycle solute may be appreciated by considering the Distal tubule
different flow rates in the vasa recta and medullary Urea
collecting duct. Although only 5% of RPF goes to the
renal medulla, this flow is much greater than the approxi- Cortex 2 H O
2
mately 3% of GFR that enters the medullary collecting Cl −
1 Na + H O 2
ducts. Consider, for example, a 10-kg dog with a GFR Outer NaCl 2
of 4 mL/min/kg and an RPF of 12 mL/min/kg. RPF medulla Urea
Cl −
in the medulla would be 6 mL/min (5% of 120), and H O Na + Urea
2
tubular fluid flow in the renal medulla would be 1.2
mL/min (3% of 40), a fivefold difference. These factors 4 5 NaCl
H O 3
2
contribute to the effective removal of water from the
Urea H 2 O
medullary interstitium and prevent dissipation of the Inner
5
osmotic gradient in this region of the kidneys. medulla NaCl NaCl NaCl Urea
Urea
ROLE OF UREA NaCl
Although there is evidence for active transport of sodium
Loop of Henle
chloride from the thick ascending limb of Henle’s loop, Collecting
tubule
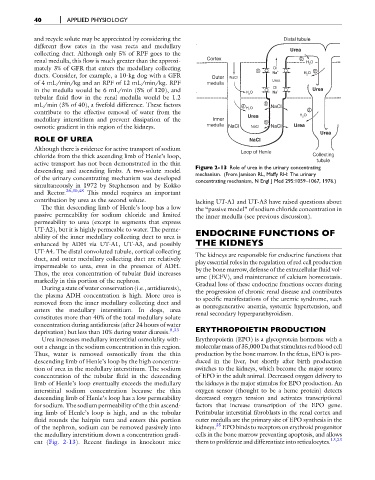
active transport has not been demonstrated in the thin Figure 2-13 Role of urea in the urinary concentrating
descending and ascending limbs. A two-solute model mechanism. (From Jamison RL, Maffy RH: The urinary
of the urinary concentrating mechanism was developed concentrating mechanism, N Engl J Med 295:1059–1067, 1976.)
simultaneously in 1972 by Stephenson and by Kokko
and Rector. 26,30,48 This model requires an important
contribution by urea as the second solute. lacking UT-A1 and UT-A3 have raised questions about
The thin descending limb of Henle’s loop has a low the “passive model” of sodium chloride concentration in
passive permeability for sodium chloride and limited the inner medulla (see previous discussion).
permeability to urea (except in segments that express
UT-A2), but it is highly permeable to water. The perme- ENDOCRINE FUNCTIONS OF
ability of the inner medullary collecting duct to urea is
enhanced by ADH via UT-A1, UT-A3, and possibly THE KIDNEYS
UT-A4. The distal convoluted tubule, cortical collecting
The kidneys are responsible for endocrine functions that
duct, and outer medullary collecting duct are relatively
play essential roles in the regulation of red cell production
impermeable to urea, even in the presence of ADH.
by the bone marrow, defense of the extracellular fluid vol-
Thus, the urea concentration of tubular fluid increases
ume (ECFV), and maintenance of calcium homeostasis.
markedly in this portion of the nephron.
Gradual loss of these endocrine functions occurs during
During a state of water conservation (i.e., antidiuresis),
the progression of chronic renal disease and contributes
the plasma ADH concentration is high. More urea is
to specific manifestations of the uremic syndrome, such
removed from the inner medullary collecting duct and
as nonregenerative anemia, systemic hypertension, and
enters the medullary interstitium. In dogs, urea renal secondary hyperparathyroidism.
constitutes more than 40% of the total medullary solute
concentration during antidiuresis (after 24 hours of water ERYTHROPOIETIN PRODUCTION
deprivation) but less than 10% during water diuresis. 8,33
Urea increases medullary interstitial osmolality with- Erythropoietin (EPO) is a glycoprotein hormone with a
out a change in the sodium concentration in this region. molecular mass of 35,000 Da that stimulates red blood cell
Thus, water is removed osmotically from the thin production by the bone marrow. In the fetus, EPO is pro-
descending limb of Henle’s loop by the high concentra- duced in the liver, but shortly after birth production
tion of urea in the medullary interstitium. The sodium switches to the kidneys, which become the major source
concentration of the tubular fluid in the descending of EPO in the adult animal. Decreased oxygen delivery to
limb of Henle’s loop eventually exceeds the medullary the kidneys is the major stimulus for EPO production. An
interstitial sodium concentration because the thin oxygen sensor (thought to be a heme protein) detects
descending limb of Henle’s loop has a low permeability decreased oxygen tension and activates transcriptional
for sodium. The sodium permeability of the thin ascend- factors that increase transcription of the EPO gene.
ing limb of Henle’s loop is high, and as the tubular Peritubular interstitial fibroblasts in the renal cortex and
fluid rounds the hairpin turn and enters this portion outer medulla are the primary site of EPO synthesis in the
35
of the nephron, sodium can be removed passively into kidneys. EPO binds to receptors on erythroid progenitor
the medullary interstitium down a concentration gradi- cells in the bone marrow preventing apoptosis, and allows
ent (Fig. 2-13). Recent findings in knockout mice them to proliferate and differentiate into reticulocytes. 13,23