
Page 42 - Small Animal Internal Medicine, 6th Edition
P. 42
14 PART I Cardiovascular System Disorders
CHF as the underlying cause. Plasma NT-proBNP between shadow in dogs with a round or barrel-shaped chest has
901-1800 pmol/L in dogs represents a “gray” zone, where greater sternal contact on lateral view and an oval shape on
VetBooks.ir increased stress on the heart is likely but CHF cannot be DV or VD view. In contrast, the heart has an upright, elon-
gated appearance on lateral view and a small, almost circular
reliably differentiated. When NT-proBNP is elevated, addi-
tional diagnostic tests (such as thoracic radiography and
Because of variations in chest conformation and the influ-
echocardiography) are recommended. Small breed dogs shape on DV or VD view in narrow- and deep-chested dogs.
with chronic mitral valve disease that have a NT-proBNP ences of respiration, cardiac cycle, and positioning on the
>1500 pmol/L are at high risk for developing CHF within the apparent size of the cardiac shadow, mild cardiomegaly may
next 12 months. An assay for canine plasma C-BNP (Cardio- be difficult to identify. Also, excess pericardial fat may mimic
BNP; ANTECH) is also available; the manufacturer reports the appearance of cardiomegaly. The cardiac shadow in
a cut-off value of 6 pg/mL as being highly sensitive and spe- puppies normally appears slightly large relative to thoracic
cific for CHF in dyspneic dogs. size compared with that of adult dogs. Radiographic sugges-
In cats, a NT-proBNP >100 pmol/L is likely to indicate tion of abnormal cardiac size or shape should be considered
increased stress or stretch on the myocardium, and follow- within the context of the physical examination and other test
up testing with echocardiography, and blood pressure and findings in all cases.
T4 (in older cats) measurement, is recommended. Hyperten- The vertebral heart score (VHS) is one widely used means
sion, hyperthyroidism, and renal dysfunction can elevate of assessing cardiomegaly in dogs and cats because there is
NT-proBNP levels. Cats with respiratory signs and a NT- good correlation between body length and heart size,
proBNP >270 pmol/L are likely to have CHF. For cats with although chest conformation may have some influence. Mea-
NT-proBNP between 100 and 269 pmol/L, respiratory signs surements for the VHS are obtained using the lateral view
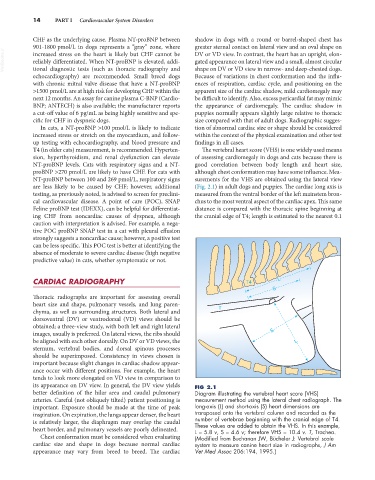
are less likely to be caused by CHF; however, additional (Fig. 2.1) in adult dogs and puppies. The cardiac long axis is
testing, as previously noted, is advised to screen for preclini- measured from the ventral border of the left mainstem bron-
cal cardiovascular disease. A point of care (POC), SNAP chus to the most ventral aspect of the cardiac apex. This same
Feline proBNP test (IDEXX), can be helpful for differentiat- distance is compared with the thoracic spine beginning at
ing CHF from noncardiac causes of dyspnea, although the cranial edge of T4; length is estimated to the nearest 0.1
caution with interpretation is advised. For example, a nega-
tive POC proBNP SNAP test in a cat with pleural effusion
strongly suggests a noncardiac cause; however, a positive test
can be less specific. This POC test is better at identifying the
absence of moderate to severe cardiac disease (high negative
predictive value) in cats, whether symptomatic or not.
CARDIAC RADIOGRAPHY T4 L
S
Thoracic radiographs are important for assessing overall
heart size and shape, pulmonary vessels, and lung paren-
chyma, as well as surrounding structures. Both lateral and T
dorsoventral (DV) or ventrodorsal (VD) views should be
obtained; a three-view study, with both left and right lateral
images, usually is preferred. On lateral views, the ribs should S
be aligned with each other dorsally. On DV or VD views, the L
sternum, vertebral bodies, and dorsal spinous processes
should be superimposed. Consistency in views chosen is
important because slight changes in cardiac shadow appear-
ance occur with different positions. For example, the heart
tends to look more elongated on VD view in comparison to
its appearance on DV view. In general, the DV view yields FIG 2.1
better definition of the hilar area and caudal pulmonary Diagram illustrating the vertebral heart score (VHS)
arteries. Careful (not obliquely tilted) patient positioning is measurement method using the lateral chest radiograph. The
important. Exposure should be made at the time of peak long-axis (L) and short-axis (S) heart dimensions are
inspiration. On expiration, the lungs appear denser, the heart transposed onto the vertebral column and recorded as the
is relatively larger, the diaphragm may overlap the caudal number of vertebrae beginning with the cranial edge of T4.
heart border, and pulmonary vessels are poorly delineated. These values are added to obtain the VHS. In this example,
L = 5.8 v, S = 4.6 v; therefore VHS = 10.4 v. T, Trachea.
Chest conformation must be considered when evaluating (Modified from Buchanan JW, Bücheler J: Vertebral scale
cardiac size and shape in dogs because normal cardiac system to measure canine heart size in radiographs, J Am
appearance may vary from breed to breed. The cardiac Vet Med Assoc 206:194, 1995.)