
Page 51 - Manual of Equine Field Surgery
P. 51
Periosteal Transection and Elevation 47
1--+--Hr-
Site of
surgical
approach
2
. "" .. , ~t:;.:f;·~-
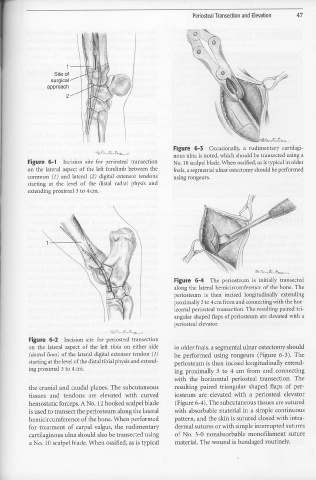
Figu re 6-3 Occasionally, a rudimentary cartilagi-
nous ulna is noted, which should be transected using a
Figure 6-1 Incision site for periosteal transection No. 10 scalpel blade. When ossified, as is typical in older
on the lateral aspect of the left forelimb between the foals, a segmental ulnar ostectomy should be performed
common (1) and lateral (2) digital extensor tendons using rongeurs.
•
starting at the level of the distal radial physis and
extending proximal 3 to 4 cm.
~ ~:G~.t,-...,.,__
Figure 6-4 The periosteum is initially transected
along the lateral hemicircumference of the bone. The
periosteum is then incised longitudinally extending
proximally 3 to 4 cm from and connecting with the hor-
izontal periosteal transection. The resulting paired tri-
angular shaped flaps of periosteum are elevated with a
periosteal elevator.
~ ('>.,,..., ~ • .1:,.<'f~~
Figure 6-2 Incision site for periosteal transection
011 the lateral aspect of the left tibia on either side in older foals, a segmental ulnar ostectomy should
( dotted lines) of the lateral digital extensor tendon (1) be performed using rongeurs (Figure 6-3). The
starting at the level of the distal tibial physis and extend- periosteum is then incised longitudinally extend-
ing proximal 3 to 4 cm. ing proximally 3 to 4 cm from and connecting
with the horizontal periosteal transection. The
the cranial and caudal planes. The subcutaneous resulting paired triangular shaped flaps of per-
tissues and tendons are elevated with curved iosteum are elevated with a periosteal elevator
hemostatic forceps. A No. 1211ooked scalpel blade (Figure 6-4). The subcutaneous tissues are sutured
is used to transect the periosteum along the lateral with absorbable material in a simple continuous
hemicircumference of the bone. When performed pattern, and the skin is sutured closed with intra-
for treatment of carpal valgus, the rudimentary dermal sutures or with simple interrupted sutures
cartilaginous ulna should also be transected using of No. 3-0 nonabsorbable monofilament suture
a No. l O scalpel blade. When ossified, as is typical material. The wound is bandaged routinely.
•